

Association of metabolic score for insulin resistance with bone mineral content and bone metabolic markers among adolescents
-
摘要:
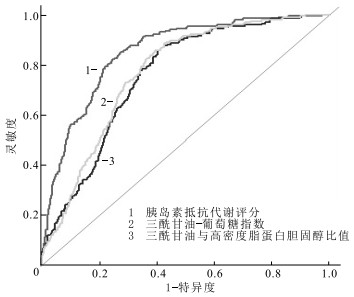
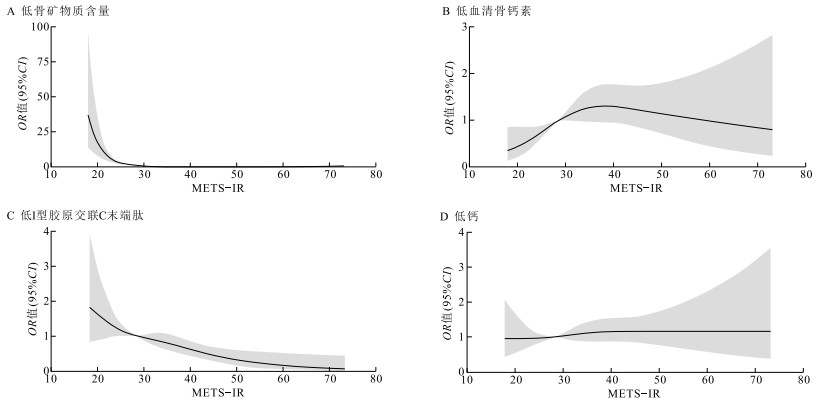
目的 分析青少年胰岛素抵抗代谢评分(METS-IR)与骨矿物质含量(BMC)、骨代谢标志物的关系,为早期识别和防治青少年骨相关疾病提供科学依据。 方法 2017—2019和2023年,通过方便抽样与分层整群随机抽样相结合的方法抽取银川市1 414名12~18岁青少年进行问卷调查、体格测量和实验室检测,以获取青少年体质量指数、BMC、血清骨钙素(OC)、Ⅰ型胶原交联C末端肽(CTX)、钙(Ca)、METS-IR等数据,根据P25、P50、P75将METS-IR分为Q1~Q4四组。使用Logistic回归模型结合限制性立方样条方法分析青少年METS-IR与BMC低下及骨代谢标志物低下的关系,通过受试者工作特征(ROC)曲线分析METS-IR对BMC低下的评估效果。 结果 青少年BMC、OC、CTX、Ca、METS-IR水平分别为(2.66±0.52)kg,(20.49±13.77)ng/mL,(2 460.89±1 818.96)pg/mL,(2.47±0.67)mmol/L,30.63±7.58;调整性别、年龄和体力活动水平后,METS-IR Q4组相较Q1组发生BMC低下和低CTX的风险降低[OR值(95%CI)分别为0.03(0.01~0.07),0.45(0.32~0.65)],发生低OC的风险升高[OR值(95%CI)=1.85(1.28~2.67)](P值均 < 0.05);性别分层后,男、女生METS-IR Q4组相较Q1组发生BMC低下、低OC和低CTX的风险与总人群相似(P值均 < 0.05);调整性别、年龄和体力活动水平后,METS-IR与BMC低下和低OC之间均存在非线性剂量-反应关系(P总趋势值均 < 0.01,P非线性值均=0.01),与低CTX存在线性剂量-反应关系(P总趋势 < 0.01,P非线性=0.72)。ROC曲线结果显示,METS-IR对BMC低下的评估效果最佳(AUC=0.85,95%CI=0.82~0.88,P < 0.01)。 结论 METS-IR评分高的学生BMC低下和低CTX的风险较低,但低OC的风险较高;且METS-IR是早期预测BMC低下的可靠指标。 Abstract:Objective To investigate the relationship of metabolic score for insulin resistance (METS-IR) with bone mineral content (BMC) and bone metabolic markers levels among adolescents, so as to provide a scientific foundation for the early identification and prevention of bone-related diseases. Methods From 2017 to 2019 and 2023, a total of 1 414 adolescents aged 12-18 years from Yinchuan were selected using a method combining convenient sampling with stratified cluster random sampling. The data of basic information, body mass index, BMC, serum osteocalcin (OC), type Ⅰ collagen cross-linked C-terminal peptide (CTX) and calcium (Ca), METS-IR among adolescents were obtained by questionnaire survey, physical measurement and laboratory examination, and METS-IR was divided into four groups Q1-Q4 according to P25, P50 and P75. Logistic regression models combined with restricted cubic splines were employed to analyze the relationship between METS-IR and low BMC as well as low bone metabolic markers. The receiver operating characteristic (ROC) curve was used to evaluate METS-IR effectiveness in diagnosing low BMC. Results The levels of BMC, OC, CTX, Ca and METS-IR in the surveyed adolescents were (2.66±0.52)kg, (20.49±13.77)ng/mL, (2 460.89±1 818.96)pg/mL, (2.47±0.67)mmol/L, 30.63±7.58. After adjusting for gender, age and physical activity level, METS-IR in Q4 group had a reduced risk of low BMC and low CTX [OR (95%CI)=0.03(0.01-0.07), 0.45(0.32-0.65)] and an elevated risk of low OC [OR (95%CI)=1.85(1.28-2.67)], compared with the Q1 group (all P < 0.05). Gender-stratified analyses revealed similar trends for both males and females (all P < 0.05). Non-linear dose-response relationships were observed between METS-IR and low BMC (Ptotal trend < 0.01, Pnon-linearity=0.01), as well as low OC (Ptotal trend < 0.01, Pnon-linearity=0.01), while a linear relationship was detected with low CTX (Ptotal trend < 0.01, Pnon-linearity=0.72). ROC curves revealed that METS-IR had the best diagnostic performance for low BMC (AUC=0.85, 95%CI=0.82-0.88, P < 0.01). Conclusions Higher METS-IR score is linked to reduced risk of low BMC and CTX but increase risk of low OC among adolescents. These findings suggest METS-IR is a reliable indicator for assessing BMC and early predicting bone health risk among adolescents. -
Key words:
- Insulin resistance /
- Bone mineral content /
- Regression analysis /
- Adolescent
1) 利益冲突声明 所有作者声明无利益冲突。 -

图 1 青少年METS-IR与骨代谢标志物低下的剂量反应关系
Figure 1. Dose-response relationship between METS-IR and low bone metabolic markers among adolescents

图 2 青少年IR替代标志物评估BMC低下的ROC曲线
Figure 2. ROC curve of IR substitution marker for evaluating low BMC among adolescents
表 1 不同性别青少年METS-TR和骨指标比较(x ±s)
Table 1. Comparison of METS-TR and bone indicators between male and female adolescents(x ±s)
性别 人数 METS-IR BMC/ kg OC/ (ng·mL-1) CTX/ (pg·mL-1) Ca/ (mmol·L-1) 男 817 30.96±7.79 2.86±0.53 22.39±14.17 2 260.42±1 698.99 2.47±0.72 女 597 30.16±7.28 2.38±0.36 17.88±12.76 2 735.24±1 939.46 2.46±0.59 合计 1 414 30.63±7.58 2.66±0.52 20.49±13.77 2 460.89±1 818.96 2.47±0.67  下载: 导出CSV
下载: 导出CSV
表 2 青少年METS-IR与骨指标的Logistic回归分析[OR值(95%CI)]
Table 2. Logistic regression analysis of METS-IR and bone indexes among adolescents[OR(95%CI)]
组别 自变量 BMC OC CTX Ca 总人群 Q2 0.28(0.19~0.43)# 1.25(0.86~1.83) 0.83(0.59~1.15) 0.84(0.60~1.17) (n=1 414) Q3 0.18(0.11~0.28)# 1.85(1.28~2.67)# 0.77(0.55~1.07) 1.05(0.76~1.45) Q4 0.03(0.01~0.07)# 1.85(1.28~2.67)# 0.45(0.32~0.65)# 1.15(0.83~1.58) 男生 Q2 0.21(0.09~0.48)# 1.35(0.77~2.38) 0.90(0.59~1.39) 1.00(0.64~1.55) (n=817) Q3 0.06(0.02~0.21)# 2.01(1.18~3.44)# 0.82(0.53~1.27) 1.04(0.67~1.60) Q4 0.05(0.01~0.17)# 1.73(1.03~2.91)# 0.55(0.36~0.85)# 1.14(0.75~1.72) 女生 Q2 0.33(0.20~0.53)# 1.21(0.73~2.01) 0.69(0.41~1.17) 0.70(0.42~1.15) (n=597) Q3 0.22(0.13~0.37)# 1.72(1.04~2.84)# 0.67(0.40~1.14) 1.05(0.65~1.70) Q4 0.02(0.01~0.07)# 2.00(1.17~3.41)# 0.29(0.14~0.57)# 1.16(0.69~1.95) 注:自变量以Q1为参照; 调整了性别、年龄、体力活动水平,#P < 0.05。
下载: 导出CSV
-
[1] LANE J M, RUSSELL L, KHAN S N. Osteoporosis[J]. Clin Orthop Relat Res, 2000, 372: 139-150. [2] MCCORMACK S E, COUSMINER D L, CHESI A, et al. Association between linear growth and bone accrual in a diverse cohort of children and adolescents[J]. JAMA Pediatr, 2017, 171(9): e171769. [3] BACHRACH L K. Hormonal contraception and bone health in adolescents[J]. Front Endocrinol, 2020(11): 603. [4] PROIA P, AMATO A, DRID P, et al. The impact of diet and physical activity on bone health in children and adolescents[J]. Front Endocrinol, 2021(12): 704647. [5] KARIMI F, RANJBAR OMRANI G, DABBAGHMANESH M H. Insulin resistance and bone health in adolescents[J]. Arch Osteoporos, 2021, 16(1): 66. [6] CONTE C, EPSTEIN S, NAPOLI N. Insulin resistance and bone: a biological partnership[J]. Acta Diabetol, 2018, 55(4): 305-314. [7] ZHANG Z, ZHAO L, LU Y, et al. Association between non-insulin-based insulin resistance indices and cardiovascular events in patients undergoing percutaneous coronary intervention: a retrospective study[J]. Cardiovasc Diabetol, 2023, 22(1): 161. [8] BORAI A, LIVINGSTONE C, KADDAM I, et al. Selection of the appropriate method for the assessment of insulin resistance[J]. BMC Med Res Methodol, 2011, 11: 158. [9] DUAN M, ZHAO X, LI S, et al. Metabolic score for insulin resistance (METS-IR) predicts all-cause and cardiovascular mortality in the general population: evidence from NHANES 2001-2018[J]. Cardiovasc Diabetol, 2024, 23(1): 243. [10] BELLO-CHAVOLLA O Y, ALMEDA-VALDES P, GOMEZ-VELASCO D, et al. METS-IR, a novel score to evaluate insulin sensitivity, is predictive of visceral adiposity and incident type 2 diabetes[J]. Eur J Endocrinol, 2018, 178(5): 533-544. [11] LIU Y, YANG Y, LI Y, et al. Nonlinear associations between METS-IR and all-cause as well as cardiovascular mortality in adults with osteoporosis and osteopenia: evidence from NHANES 2007-2023[J]. Sci Rep, 2025, 15(1): 12657. [12] LI M, GAO L, LIU Y, et al. Relationship between insulin resistance surrogates and bone mineral density in postmenopausal women[J]. Climacteric, 2025, 28(2): 154-161. [13] PU B, GU P, YUE D, et al. The METS-IR is independently related to bone mineral density, FRAX score, and bone fracture among U.S. non-diabetic adults: a cross-sectional study based on NHANES[J]. BMC Musculoskelet Disord, 2023, 24(1): 730. [14] 周金玉, 白玲, 佟玲玲, 等. 银川市青少年体脂肪分布与骨矿物质含量的关系[J]. 中国学校卫生, 2022, 43(9): 1376-1379.ZHOU J Y, BAI L, TONG L L, et al. Relationship between body fat distribution and bone mineral content of adolescents in Yinchuan[J]. Chin J Sch Health, 2022, 43(9): 1376-1379. (in Chinese) [15] FEWTRELL M S. Bone densitometry in children assessed by dual X ray absorptiometry: uses and pitfalls[J]. Arch Dis Child, 2003, 88(9): 795-798. [16] FULZELE K, RIDDLE R C, DIGIROLAMO D J, et al. Insulin receptor signaling in osteoblasts regulates postnatal bone acquisition and body composition[J]. Cell, 2010, 142(2): 309-319. [17] PRAMOJANEE S N, PHIMPHILAI M, CHATTIPAKORN N, et al. Possible roles of insulin signaling in osteoblasts[J]. Endocr Res, 2014, 39(4): 144-151. [18] 张丽, 卜淑敏. 肥胖对骨骼的双重影响和机制以及在骨疾病中的作用[J]. 中国骨质疏松杂志, 2022, 28(4): 585-589.ZHANG L, PU S M. The dual effects and mechanisms of obesity on bone and its roles in bone diseases[J]. Chin J Osteoporos, 2022, 28(4): 585-589. (in Chinese) [19] TIAN W, TENG F, GAO J, et al. Estrogen and insulin synergistically promote endometrial cancer progression via crosstalk between their receptor signaling pathways[J]. Cancer Biol Med, 2019, 16(1): 55-70. [20] KALIMERI M, LEEK F, WANG N X, et al. Association of insulin resistance with bone strength and bone turnover in menopausal Chinese-Singaporean women without diabetes[J]. Int J Environ Res Public Health, 2018, 15(5): 889. [21] KHANMOHAMMADI S, KUCHAY M S. Effects of metabolic dysfunction-associated steatotic liver disease on bone density and fragility fractures: associations and mechanisms[J]. J Obes Metab Syndr, 2024, 33(2): 108-120. [22] HUANG H, WANG A, CONG L, et al. Osteocalcin is associated with triglyceride glucose index rather than HOMA-IR in men with type 2 diabetes[J]. Front Endocrinol, 2022, 13: 1067903. [23] BILOTTA F L, ARCIDIACONO B, MESSINEO S, et al. Insulin and osteocalcin: further evidence for a mutual cross-talk[J]. Endocrine, 2018, 59(3): 622-632. [24] OSTA B, BENEDETTI G, MIOSSEC P. Classical and paradoxical effects of TNF-α on bone homeostasis[J]. Front Immunol, 2014, 5: 48. [25] MA C, TONKS K T, CENTER J R, et al. Complex interplay among adiposity, insulin resistance and bone health[J]. Clin Obes, 2018, 8(2): 131-139. [26] LIU X Z, FAN J, PAN S J. METS-IR, a novel simple insulin resistance indexes, is associated with hypertension in normal-weight Chinese adults[J]. J Clin Hypertens, 2019, 21(8): 1075-1081. [27] ZHANG M, LIU D, QIN P, et al. Association of metabolic score for insulin resistance and its 6-year change with incident type 2 diabetes mellitus[J]. J Diabetes, 2021, 13(9): 725-734. -

 点击查看大图
点击查看大图
计量
- 文章访问数: 8
- HTML全文浏览量: 7
- PDF下载量: 0
- 被引次数: 0