


Association of cysteine level and bone mineral density among children with cerebral palsy
-
摘要:
目的 了解脑瘫患儿血清同型半胱氨酸水平和腰椎骨密度(BMD)现况并分析两者的关联性,为改善脑瘫患儿骨健康提供参考。 方法 2023年1月—2024年1月选取G市社会福利院(萝岗院区)的149名10~18岁脑瘫患儿,通过福利院病案系统导出脑瘫患儿基本人口学信息,采用酶循环法测量患儿血清同型半胱氨酸水平,由专业康复医师使用双能X线吸收法对患儿腰椎BMD进行测定,并计算腰椎身高校正BMD Z值(BMD HAZ值)。采用非限制性立方样条和分段多重线性回归分别分析脑瘫患儿血清同型半胱氨酸水平与腰椎BMD HAZ值的关联性。 结果 脑瘫患儿血清同型半胱氨酸浓度中位数为9.13(8.42,10.30)μmol/L,痉挛型脑瘫患儿浓度[9.28(8.53, 10.49)μmol/L]高于非痉挛型[8.64(7.89, 9.66)μmol/L](Z=-2.46,P < 0.05)。腰椎BMD HAZ值中位数为-1.07(-2.10,-0.16),脑瘫患儿低BMD检出率为29.5%。脑瘫患儿血清同型半胱氨酸浓度与腰椎BMD HAZ值呈“L”型关联。当血清同型半胱氨酸浓度≤8.7 μmol/L时,腰椎BMD HAZ值与血清同型半胱氨酸浓度呈负相关(B=-0.32,95%CI=-1.06~-0.15,P < 0.05)。 结论 脑瘫患儿在较低血清同型半胱氨酸浓度下发现与腰椎BMD的负相关,提示其对同型半胱氨酸影响的敏感性可能较健康儿童青少年高,即使未达到高同型半胱氨酸血症标准也应引起重视。 Abstract:Objective To investigate the association between cysteine level and lumbar spine (LS) bone mineral density (BMD) among children with cerebral palsy, so as to provide a basis for bone health enhancement among children with cerebral palsy. Methods A total of 149 children aged 10-18 with cerebral palsy who were admitted to the G city Social Welfare Institute (Luogang District) from January 2023 to January 2024. Basic demographic characteristics of children with cerebral palsy were extracted from medical records system. Cysteine levels were measured using the enzyme cycling method. LS BMD of the children was determined by specialized rehabilitation physicians using dual-energy X-ray absorptiometry, and the corrected BMD Z-scores for LS were calculated. Non-restrictive cubic splines and segmented multiple linear regression were employed to analyze the correlation between cysteine levels and age-specific height Z-scores (HAZ-scores) for LS BMD in children with cerebral palsy. Results The median cysteine concentration in children with cerebral palsy was 9.13(8.42, 10.30)μmol/L, with significantly higher levels in spastic type children [9.28(8.53, 10.49)μmol/L] compared to non-spastic types [8.64(7.89, 9.66)μmol/L](Z=-2.46, P < 0.05). The median LS BMD HAZ-score was -1.07(-2.10, -0.16), and the detection rate of decreased bone mass was 29.5%. There was an "L"-shaped association between serum homocysteine concentration and LS BMD HAZ-score in children with cerebral palsy. When serum homocysteine concentration was below 8.7 μmol/L, a significant negative correlation was observed between LS BMD HAZ-score and serum homocysteine concentration (B=-0.32, 95%CI=-1.06 to -0.15, P < 0.05). Conclusions The significant negative correlation between cysteine levels and LS BMD in children with cerebral palsy at lower cysteine concentrations, which suggests a potentially higher sensitivity to the influence of homocysteine than healthy children and adolescents, warranting attention even if not reaching the standard of hyperhomocysteinemia. -
Key words:
- Cerebral Palsy /
- Cysteine /
- Bone density /
- Regression analysis /
- Child
1) 利益冲突声明 所有作者声明无利益冲突。 -

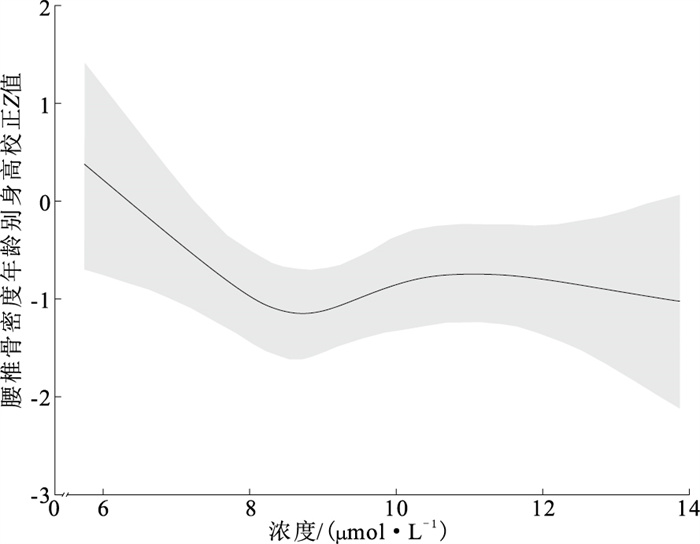
图 1 脑瘫患儿血清Hcy浓度与LS BMD HAZ值RCS曲线
Figure 1. RCS curve of serum Hcy and LS BMD HAZ score among children with cerebral palsy
表 1 不同组别脑瘫患儿血清Hcy水平比较[M(P25, P75), μmol/L]
Table 1. Comparison of the serum Hcy concentration in children with cerebral palsy [M(P25, P75), μmol/L]
组别 选项 人数 血清Hcy水平 Z/H值 P值 年龄/岁 11~12 23 8.81(8.31, 9.87) 3.57 0.31 13~14 43 9.11(8.59, 10.21) 15~16 48 9.09(8.30, 10.17) 17~18 35 9.46(8.53, 10.59) 性别 男 86 9.01(8.30, 10.30) -0.75 0.45 女 63 9.28(8.57, 10.32) BMI 正常 36 8.96(8.26, 10.29) -0.52 0.60 消瘦 113 9.14(8.45, 10.30) 脑瘫分型 痉挛型 115 9.28(8.53, 10.49) -2.46 < 0.05 非痉挛型 34 8.64(7.89, 9.66) GMFCS分级 轻度 32 8.89(8.38, 10.21) -0.66 0.51 中重度 117 9.19(8.43, 10.38) 25-羟基维生 正常 132 9.08(8.40, 10.21) -1.56 0.12 素D水平 不足/缺乏 17 10.21(8.95, 10.55) 叶酸水平 正常 138 9.10(8.41, 10.24) -1.51 0.13 缺乏 11 10.13(8.61, 10.80) 吞咽功能障碍 是 40 9.27(8.02, 10.45) -0.31 0.76 否 109 9.09(8.49, 10.25) 癫痫 是 44 9.16(8.48, 10.23) -0.03 0.96 否 105 9.11(8.38, 10.51)  下载: 导出CSV
下载: 导出CSV
表 2 不同组别脑瘫患儿腰椎BMD HAZ评分比较[M(P25, P75)]
Table 2. Comparison of lumbar BMD HAZ score in children with cerebral palsy [M(P25, P75)]
组别 选项 人数 统计值 L1 L2 L3 L4 LS BMD 年龄/岁 11~12 23 -0.80(-1.50, -0.34) -1.17(-1.93, -0.39) -1.37(-1.81, -0.37) -0.97(-1.59, -0.17) -1.07(-1.80, -0.47) 13~14 43 -1.34(-1.87, -0.43) -1.27(-2.51, -0.53) -1.15(-2.30, -0.45) -1.13(-2.20, -0.20) -1.25(-2.65, -0.55) 15~16 48 -0.50(-1.58, 0.18) -0.79(-1.68, 0.24) -0.91(-1.91, 0.13) -0.63(-1.79, 0.01) -0.89(-2.10, 0.02) 17~18 35 -0.34(-1.49, 0.41) -0.13(-1.65, 0.48) -0.21(-1.76, 0.41) -0.62(-1.75, 0.06) -0.42(-2.05, 0.21) H值 6.09* 9.91* 5.22 2.12 3.16 性别 男 86 -0.62(-1.35, 0.20) -0.66(-1.32, 0.24) -0.63(-1.43, 0.16) -0.59(-1.32, 0.06) -0.74(-1.47, 0.13) 女 63 -1.36(-2.18, -0.34) -1.84(-2.79, -0.25) -1.77(-2.86, -0.37) -1.60(-2.62, -0.15) -2.16(-3.00, -0.27) Z值 -3.32* -4.35** -4.28** -3.79** -4.37** BMI 正常 36 -0.34(-1.22, 0.55) -0.20(-1.23, 0.53) -0.09(-1.57, 0.46) -0.06(-1.01, 0.63) -0.22(-1.44, 0.32) 消瘦 113 -1.05(-1.78, -0.25) -1.17(-2.01, -0.21) -1.27(-1.96, -0.28) -1.13(-1.94, -0.26) -1.26(-2.25, -0.45) Z值 -2.77* -3.06* -3.06* -3.79* -3.34* 脑瘫分型 痉挛型 115 -1.00(-1.77, -0.06) -1.10(-1.93, 0.06) -1.15(-1.95, -0.04) -1.11(-1.98, -0.15) -1.26(-2.25, -0.24) 非痉挛型 34 -0.56(-1.35, -0.02) -0.71(-1.38, 0.01) -0.59(-1.45, 0.37) -0.41(-1.21, 0.48) -0.68(-1.45, 0.25) Z值 -1.31 -1.31 -1.73 -2.38* -1.97* GMFCS分级 轻度 32 -0.40(-1.32, 0.32) -0.62(-1.30, 0.27) -0.53(-1.41, 0.41) -0.22(-1.18, 0.46) -0.57(-1.31, 0.27) 中重度 117 -0.84(-1.78, -0.07) -1.06(-2.03, -0.05) -1.15(-1.97, -0.06) -1.10(-2.01, -0.19) -1.26(-2.27, -0.27) Z值 -1.95 -2.13* -2.00* -2.69* -2.67* 维生素D 正常 132 -0.78(-1.64, -0.03) -0.80(-1.92, 0.06) -0.88(-1.89, 0.08) -0.92(-1.76, -0.04) -1.00(-2.13, -0.05) 水平 不足/缺乏 17 -1.32(-1.85, -0.36) -1.22(-2.04, -0.41) -1.33(-2.03, -0.56) -1.18(-1.81, -0.25) -1.38(-2.13, -0.51) Z值 -1.16 -0.98 -1.06 -0.62 -1.00 叶酸水平 正常 138 -0.82(-1.65, -0.08) -0.92(-1.92, -0.07) -0.99(-1.87, 0.03) -0.95(-1.74, -0.08) -1.14(-2.01, -0.21) 缺乏 11 -0.43(-1.62, 0.79) 0.07(-2.52, 0.59) -0.37(-2.72, 0.19) -0.21(-2.62, -0.03) -0.41(-2.82, 0.29) Z值 -0.81 -0.77 -0.22 -0.08 -0.39 吞咽功能 是 40 -1.39(-2.25, -0.29) -1.57(-2.81, -0.40) -1.53(-2.82, -0.52) -1.51(-2.32, -0.27) -1.72(-3.17, -0.60) 障碍 否 109 -0.76(-1.42, 0.04) -0.74(-1.73, 0.16) -0.75(-1.77, 0.17) -0.72(-1.62, 0.06) -0.82(-1.83, 0.08) Z值 -2.34* -3.17* -2.87* -3.00* -3.01* 癫痫 是 44 -1.16(-1.70, -0.01) -1.05(-1.93, -0.12) -1.16(-1.75, -0.11) -0.99(-1.52, -0.17) -1.24(-1.80, -0.41) 否 105 -0.77(-1.64, -0.06) -0.86(-1.90, 0.07) -0.85(-1.97, 0.17) -0.90(-1.87, 0.02) -0.99(-2.26, 0.04) Z值 -0.73 -0.43 -0.21 -0.17 -0.31 总体 149 -0.80(-1.64, -0.06) -0.87(-1.92, 0.05) -0.97(-1.91, 0.05) -0.94(-1.76, -0.07) -1.07(-2.10, -0.16) 注:*P < 0.05,**P < 0.01。
下载: 导出CSV
表 3 脑瘫患儿血清Hcy水平与LS BMD HAZ值关联性多重线性回归分析[B值(95% CI), n=149]
Table 3. Segmented multiple linear regression of serum Hcy with LS BMD HAZ score among children with cerebral palsy[B(95% CI), n=149]
变量 选项 Hcy≤8.7 μmol/L Hcy>8.7 μmol/L 年龄/岁 11~14 -0.41(-1.22~-0.07)* 0.15(-0.15~0.57) 15~18 -0.29(-1.63~0.28) 0.08(-0.20~0.37) 性别 男 -0.26(-0.92~0.13) -0.09(-0.30~0.16) 女 -0.55(-2.42~0.06) 0.23(-0.09~0.75) BMI 正常 -0.71(-3.81~1.35) 0.23(-0.30~0.74) 消瘦 -0.34(-1.28~-0.12)* 0.19(-0.04~0.43) 脑瘫分型 痉挛型 -0.35(-1.26~-0.09)* 0.04(-0.18~0.28) 非痉挛型 -0.32(-2.00~0.84) 0.35(-1.03~2.01) GMFCS分级 轻度 -0.37(-2.05~0.78) -0.01(-0.81~0.80) 中重度 -0.34(-1.16~-0.18)* 0.06(-0.17~0.31) 维生素D水平 不足/缺乏 — 0.05(-0.19~0.30) 正常 -0.34(-1.10~-0.20)* -0.55(-2.88~1.23) 叶酸水平 缺乏 — — 正常 -0.34(-1.06~-0.21)* 0.01(-0.20~0.22) 吞咽功能障碍 是 -0.12(-1.37~0.92) 0.19(-0.31~0.80) 否 -0.29(-1.16~0.05) -0.01(-0.25~0.24) 癫痫 是 -0.30(-1.88~0.54) 0.15(-0.14~0.45) 否 -0.34(-1.24~-0.04)* 0.09(-0.15~0.38) 总体 -0.32(-1.06~-0.15)* 0.06(-0.15~0.28) 注:* P < 0.05。
下载: 导出CSV
-
[1] COLVER A, FAIRHURST C, PHAROAH P O. Cerebral palsy[J]. Lancet, 2014, 383(9924): 1240-1249. doi: 10.1016/S0140-6736(13)61835-8 [2] DEMAURO S B, MCDONALD S A, HEYNE R J, et al. Increasing prevalence of cerebral palsy among two-year-old children born at < 27 weeks of Gestation: a cohort study[J]. J Pediatr, 2024, 268: 113944. doi: 10.1016/j.jpeds.2024.113944 [3] 封玉霞, 庞伟, 李鑫, 等. 中国0~6岁儿童脑瘫患病率的Meta分析[J]. 中国全科医学, 2021, 24(5): 603-607.FENG Y X, PANG W, LI X, et al. The prevalence of cerebral palsy in children aged 0-6 years in China: a Meta-analysis[J]. Chin Gen Pract, 2021, 24(5): 603-607. (in Chinese) [4] NAUME M M, JØRGENSEN M H, HØI-HANSEN C E, et al. Low skeletal muscle mass and liver fibrosis in children with cerebral palsy[J]. Eur J Pediatr, 2023, 182(11): 5047-5055. doi: 10.1007/s00431-023-05177-9 [5] GRANILD-JENSEN J B, PEDERSEN A B, KRISTIANSEN E B, et al. Fracture rates in children with cerebral palsy: a danish, nationwide register-based study[J]. Clin Epidemiol, 2022, 14: 1405-1414. doi: 10.2147/CLEP.S381343 [6] WHITNEY D G. 5-year fracture risk among children with cerebral palsy[J]. Pediatr Res, 2023, 93(4): 996-1002. doi: 10.1038/s41390-022-02207-4 [7] LI X, ZHOU Z, TAO Y, et al. Linking homocysteine and ferroptosis in cardiovascular disease: insights and implications[J]. Apoptosis, 2024. DOI: 10.1007/s10495-024-01999-6. [8] REHACKOVA P, SKALOVA S, KUTILEK S. Serum homocysteine levels in children and adolescents with impaired bone health[J]. Rev Bras Reumatol, 2013, 53(6): 464-468. doi: 10.1016/j.rbr.2013.06.001 [9] 吕海宏, 汤旭磊, 傅松波, 等. 同型半胱氨酸调控成骨细胞增殖分化的分子机制研究[C]//中华医学会第十二次全国内分泌学学术会议论文汇编, 西安, 2013.LV H H, TANG X L, FU S B, et al. Molecular mechanism of homocysteine regulation of osteoblast proliferation and differentiation[C]//Proceedings of the 12th National Endocrinology Academic Conference of the Chinese Medical Association, Xi'an, 2013. (in Chinese) [10] KIM H J, CHANG E J, KIM H M, et al. Antioxidant alpha-lipoic acid inhibits osteoclast differentiation by reducing nuclear factor-kappa B DNA binding and prevents in vivo bone resorption induced by receptor activator of nuclear factor-kappa B ligand and tumor necrosis factor-alpha[J]. Free Radic Biol Med, 2006, 40(9): 1483-1493. doi: 10.1016/j.freeradbiomed.2005.10.066 [11] WEISS N, HEYDRICK S, ZHANG Y Y, et al. Cellular redox state and endothelial dysfunction in mildly hyperhomocysteinemic cystathionine beta-synthase-deficient mice[J]. Arterioscler Thromb Vasc Biol, 2002, 22(1): 34-41. doi: 10.1161/hq1201.100456 [12] 中国康复医学会儿童康复专业委员会, 中国残疾人康复协会小儿脑性瘫痪康复专业委员会, 中国医师协会康复医师分会儿童康复专业委员会, 等. 中国脑性瘫痪康复指南(2022)第一章: 概论[J]. 中华实用儿科临床杂志, 2022, 37(12): 887-892.Chinese Association of Rehabilitation Medicine Pediatric Rehabilitation Committee, Chinese Association of Rehabilitation of Disabled Persons Rehabilitation Committee for Pediatric Cerebral Palsy, Chinese Medical Doctor Association Pediatric Rehabilitation Rehabilitation Committee, et al. Chinese rehabilitation guidelines for cerebral palsy (2022) part 1: overview[J]. Chin J Appl Clin Pediatr, 2022, 37(12): 887-892. (in Chinese) [13] STEVENSON R D. Use of segmental measures to estimate stature in children with cerebral palsy[J]. Arch Pediatr Adolesc Med, 1995, 149(6): 658-662. doi: 10.1001/archpedi.1995.02170190068012 [14] PALISANO R, ROSENBAUM P, WALTER S, et al. Development and reliability of a system to classify gross motor function in children with cerebral palsy[J]. Dev Med Child Neurol, 1997, 39(4): 214-223. doi: 10.1111/j.1469-8749.1997.tb07414.x [15] 中华人民共和国国家卫生和计划生育委员会. 学龄儿童青少年营养不良筛查: WS/T 456—2014[S]. 2014-12-15.National Health and Family Planning Commission of the PRC. Screening standard for malnutrition of school-age children and adolescent: WS/T 456-2014[S]. 2014-12-15. [16] 中华人民共和国国家卫生和计划生育委员会. 学龄儿童青少年超重与肥胖筛查: WS/T 586—2018[S]. 2018-08-01.National Health and Family Planning Commission of the PRC. Screening for overweight and obesity among school-age children and adolescents: WS/T 586-2018[S]. 2018-08-01. (in Chinese) [17] 中华人民共和国国家卫生健康委员会. 人群维生素D缺乏筛査方法: WS/T 677—2020[S]. 2020-11-01.National Health Commission of the PRC. Method for vitamin D deficiency screening: WS/T 677-2020[S]. 2020-11-01. (in Chinese) [18] BRUNO D B. Conclusions of a WHO technical consultation on folate and vitamin B12 deficiencies[J]. Food Nutr Bull, 2008, 29(2): S238-S244. [19] CRABTREE N J, ARABI A, BACHRACH L K, et al. Dual-energy X-ray absorptiometry interpretation and reporting in children and adolescents: the revised 2013 ISCD Pediatric Official Positions[J]. J Clin Densitom, 2014, 17(2): 225-242. doi: 10.1016/j.jocd.2014.01.003 [20] ZONG X N, LI H. Construction of a new growth references for China based on urban Chinese children: comparison with the WHO growth standards[J]. PLoS One, 2013, 8(3): e59569. doi: 10.1371/journal.pone.0059569 [21] 彭晓音. 脊髓性肌萎缩症患儿骨密度状况及其影响因素分析[D]. 北京: 北京协和医学院, 2022.PENG X Y. Bone mineral density status and its influencing factors in children with spinal muscular atrophy[D]. Beijing: Peking Union Medical College, 2022. (in Chinese) [22] TOSUN A, ERISEN KARACA S, UNUVAR T, et al. Bone mineral density and vitamin D status in children with epilepsy, cerebral palsy, and cerebral palsy with epilepsy[J]. Childs Nerv Syst, 2017, 33(1): 153-158. doi: 10.1007/s00381-016-3258-0 [23] RODEN R C, NORITZ G, MCKNIGHT E R, et al. An exploratory study of depot-medroxyprogesterone acetate and bone mineral density in adolescent and young adult women with cerebral palsy[J]. Contraception, 2020, 101(4): 273-275. doi: 10.1016/j.contraception.2019.12.009 [24] JUNG K J, KWON S S, CHUNG C Y, et al. Association of gross motor function classification system level and school attendance with bone mineral density in patients with cerebral palsy[J]. J Clin Densitom, 2018, 21(4): 501-506. doi: 10.1016/j.jocd.2016.09.002 [25] FINBRÅTEN A K, SYVERSEN U, SKRANES J, et al. Bone mineral density and vitamin D status in ambulatory and non-ambulatory children with cerebral palsy[J]. Osteoporos Int, 2015, 26(1): 141-150. doi: 10.1007/s00198-014-2840-0 [26] RUIZ BRUNNER M L M, CUESTAS E, HEINEN F, et al. Growth in infants, children and adolescents with unilateral and bilateral cerebral palsy[J]. Sci Rep, 2022, 12(1): 1879. doi: 10.1038/s41598-022-05267-y [27] ZEMEL B S, LEONARD M B, KELLY A, et al. Height adjustment in assessing dual energy X-ray absorptiometry measurements of bone mass and density in children[J]. J Clin Endocrinol Metab, 2010, 95(3): 1265-1273. doi: 10.1210/jc.2009-2057 [28] SCHOENDORFER N C, OBEID R, MOXON-LESTER L, et al. Methylation capacity in children with severe cerebral palsy[J]. Eur J Clin Invest, 2012, 42(7): 768-776. doi: 10.1111/j.1365-2362.2011.02644.x [29] MARON B A, LOSCALZO J. The treatment of hyperhomocysteinemia[J]. Annu Rev Med, 2009, 60: 39-54. doi: 10.1146/annurev.med.60.041807.123308 [30] REFSUM H, SMITH A D, UELAND P M, et al. Facts and recommendations about total homocysteine determinations: an expert opinion[J]. Clin Chem, 2004, 50(1): 3-32. doi: 10.1373/clinchem.2003.021634 [31] MINIKSAR D Y, CANSLZ M A, KLLLŞ M, et al. Relationship between sleep problems and chronotypes of children and adolescents with attention deficit and hyperactivity disorder and serum GABA, glutamate and homocysteine levels[J]. Chronobiol Int, 2022, 39(3): 386-397. doi: 10.1080/07420528.2021.2018452 [32] GONZÁLEZ-JIMÉNEZ E, MONTERO-ALONSO M A, SCHMIDT-RIOVALLE J, et al. Metabolic syndrome in Spanish adolescents and its association with birth weight, breast feeding duration, maternal smoking, and maternal obesity: a cross-sectional study[J]. Eur J Nutr, 2015, 54(4): 589-597. doi: 10.1007/s00394-014-0740-x [33] CHUNG K H, CHIOU H Y, CHEN Y H. Associations between serum homocysteine levels and anxiety and depression among children and adolescents in Taiwan[J]. Sci Rep, 2017, 7(1): 8330. doi: 10.1038/s41598-017-08568-9 [34] FU L, WANG Y, HU Y Q. Inferring causal effects of homocysteine and B-vitamin concentrations on bone mineral density and fractures: Mendelian randomization analyses[J]. Front Endocrinol (Lausanne), 2022, 13: 1037546. doi: 10.3389/fendo.2022.1037546 [35] FLEISS B, GRESSENS P. Tertiary mechanisms of brain damage: a new hope for treatment of cerebral palsy?[J]. Lancet Neurol, 2012, 11(6): 556-566. doi: 10.1016/S1474-4422(12)70058-3 [36] LIN C Y, CHANG Y C, WANG S T, et al. Altered inflammatory responses in preterm children with cerebral palsy[J]. Ann Neurol, 2010, 68(2): 204-212. doi: 10.1002/ana.22049 [37] VAES B L, LUTE C, BLOM H J, et al. Vitamin B12 deficiency stimulates osteoclastogenesis via increased homocysteine and methylmalonic acid[J]. Calcif Tissue Int, 2009, 84(5): 413-422. doi: 10.1007/s00223-009-9244-8 [38] HERRMANN M, WIDMANN T, COLAIANNI G, et al. Increased osteoclast activity in the presence of increased homocysteine concentrations[J]. Clin Chem, 2005, 51(12): 2348-2353. doi: 10.1373/clinchem.2005.053363 [39] KANAZAWA I, TOMITA T, MIYAZAKI S, et al. Bazedoxifene ameliorates homocysteine-induced apoptosis and accumulation of advanced glycation end products by reducing oxidative stress in MC3T3-E1 Cells[J]. Calcif Tissue Int, 2017, 100(3): 286-297. doi: 10.1007/s00223-016-0211-x [40] MILLS E L, KELLY B, O'NEILL L A J. Mitochondria are the powerhouses of immunity[J]. Nat Immunol, 2017, 18(5): 488-498. doi: 10.1038/ni.3704 [41] PHULL A R, NASIR B, HAQ I U, et al. Oxidative stress, consequences and ROS mediated cellular signaling in rheumatoid arthritis[J]. Chem Biol Interact, 2018, 281: 121-136. doi: 10.1016/j.cbi.2017.12.024 [42] DEODATI A, MANCO M, MARIANI M, et al. Bone density and body composition in small for gestational age children with adequate catch up growth: a preliminary retrospective case control study[J]. Bone, 2021, 153: 116114. doi: 10.1016/j.bone.2021.116114 -

 点击查看大图
点击查看大图
计量
- 文章访问数: 222
- HTML全文浏览量: 94
- PDF下载量: 17
- 被引次数: 0