


Disease burden and prediction of attention deficit hyperactivity disorder in Chinese children and adolescents from 1990 to 2019
-
摘要:
目的 了解1990—2019年中国儿童青少年注意缺陷多动障碍(ADHD)疾病负担情况及发展趋势,为卫生行政部门制定政策提供基础理论依据。 方法 利用2019年全球疾病负担数据库,分析不同性别及年龄组ADHD的发病率、患病率及伤残调整寿命年(DALY)率,并对ADHD疾病趋势进行预测。 结果 2019年中国的ADHD发病率、患病率和DALY率分别为70.41/10万、1 546.15/10万和18.87/10万,与1990年相比分别降低27.30%,25.35%和55.80%,并且女性均低于男性。2019年5~9岁年龄组ADHD发病率最高,为837.76/10万,而患病率和DALY率最高的年龄组均为10~14岁组,分别为5 740.47/10万和70.49/10万。Joinpoint回归模型结果显示,1990—2019年ADHD发病率、患病率和DALY率均有降低趋势,平均年度变化百分比(AAPC)分别为-1.35%,-1.16%和-1.16%,差异均有统计学意义(P值均<0.05)。灰色预测模型GM(1, 1)预测结果显示,2020—2030年中国ADHD的发病率和患病率均呈下降趋势。 结论 1990—2019年中国ADHD疾病负担呈降低趋势,中国对儿童青少年ADHD的防治效果有效。应继续采取积极的预防措施以减轻儿童青少年人群ADHD的疾病负担。 -
关键词:
- 注意力缺陷障碍伴多动 /
- 患病代价 /
- 回归分析 /
- 儿童 /
- 青少年
Abstract:Objective To analyze the disease burden and trend of attention deficit hyperactivity disorder (ADHD) in China from 1990 to 2019, so as to provide the basic theoretical basis for the health administrative departments to formulate policies. Methods Using the 2019 Global Burden of Disease Database, the incidence, prevalence and disability adjusted life year (DALY) rates of ADHD were analyzed for both sex and different age groups, and the trends of ADHD were predicted. Results In 2019, the incidence, prevalence and DALY rate of ADHD in China were 70.41/100 000, 1 546.15/100 000 and 18.87/100 000 respectively. Compared with 1990, the rates decreased by 27.30%, 25.35% and 55.80% respectively, and these rates of females were lower than those of males. In 2019, the incidence rate of ADHD was the highest in the age group 5-9 years old (837.76/100 000), while the highest prevalence and DALY rates were found in ages groups of 10-14 years old (5 740.47/100 000 and 70.49/100 000). The results of the Joinpoint regression model showed that the incidence, prevalence and DALY rate had a downward trend from 1990 to 2019. The AAPC was -1.35%, -1.16% and -1.16%, respectively, with a statistically significant difference (P < 0.05). The prediction results of grey prediction model GM (1, 1) indicated that the incidence and prevalence rate of ADHD in China would decline from 2020 to 2030. Conclusion The burden of ADHD in China showed a decreasing trend from 1990 to 2019, indicating that the prevention and treatment effect of ADHD in children and adolescents of China was effective. China should take active preventive measures to reduce the burden of ADHD in children and adolescents. -
Key words:
- Attention deficit disorder with hyperactivity /
- Cost of illness /
- Regression /
- Child /
- Adolescent
1) 利益冲突声明 所有作者声明无利益冲突。 -

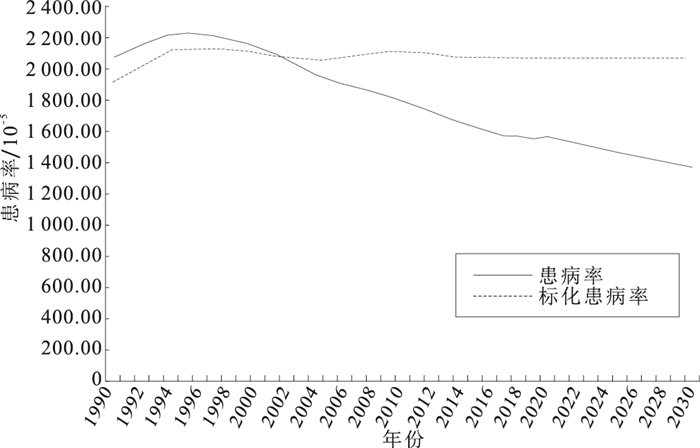
图 1 预测2020—2030年ADHD发病率和标化发病率
Figure 1. Prediction of ADHD incidence rate and standardized incidence rate during 2020-2030

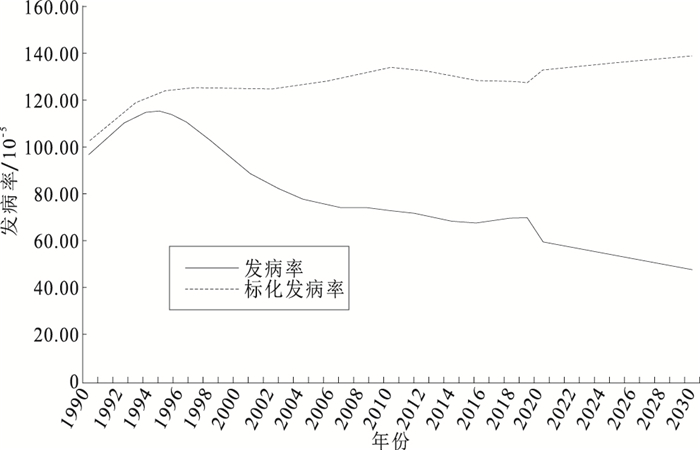
图 2 预测2020—2030年ADHD患病率和标化患病率
Figure 2. Prediction of ADHD prevalence rate and standardized prevalence rate during 2020-2030
表 1 中国1990和2019年儿童青少年ADHD疾病负担情况/10-5
Table 1. Disease burden of ADHD in Chinese children and adolescents in 1990 and 2019/10-5
组别 年份 发病率 标化发病率 患病率 标化患病率 DALY率 标化DALY率 男 1990 142.15 148.55 2 955.79 2 717.48 36.13 33.21 2019 105.55 180.32 2 227.29 2 900.36 27.21 35.51 女 1990 48.68 52.30 1 129.99 1 039.44 13.74 12.63 2019 33.89 65.45 835.35 1 134.77 10.20 13.86 合计 1990 96.86 102.57 2 071.19 1 906.92 42.70 23.27 2019 70.41 127.47 1 546.15 2 070.84 18.87 25.34  下载: 导出CSV
下载: 导出CSV
表 2 不同年龄组儿童青少年1990和2019年ADHD疾病负担情况/10-5
Table 2. Burden of ADHD in different age groups in Chinese adolescents and children in 1990 and 2019/10-5
年龄组/岁 年份 发病率 患病率 DALY率 男性 女性 合计 男性 女性 合计 男性 女性 合计 <5 1990 476.76 164.45 329.36 495.84 171.21 342.62 6.10 2.11 4.21 2019 596.79 211.00 418.70 620.48 219.65 435.44 7.63 2.72 5.36 5~9 1990 976.44 347.09 674.38 5 213.21 1 828.88 3 588.87 64.05 22.46 44.09 2019 1 181.18 433.62 837.76 6 289.08 2 275.25 4 445.16 77.33 28.02 54.68 10~14 1990 84.82 30.44 58.51 6 922.91 2 486.42 4 776.49 84.92 30.47 58.57 2019 102.86 38.24 73.29 8 038.79 3 015.30 5 740.47 98.72 37.03 70.49 15~19 1990 0 0 0 5 515.09 2 087.21 3 847.60 67.58 25.46 47.09 2019 0 0 0 5 821.74 2 312.50 4 185.18 71.39 28.27 51.29
下载: 导出CSV
表 3 中国1990—2019年儿童青少年ADHD疾病负担趋势分析/10-5
Table 3. Analysis of disease burden trend of ADHD in Chinese children and adolescents from 1990 to 2019/10-5
指标 趋势1 趋势2 趋势3 整体趋势 年份 APC(95%CI) 年份 APC(95%CI) 年份 APC(95%CI) 年份 AAPC(95%CI) 发病率 1990—1995 3.72(2.62~4.74)* 1995—2004 -4.74(-5.14~-4.20)* 2004—2019 -0.94(-1.15~-0.74)* 1990—2019 -1.35(-1.55~-1.14)* 患病率 1990—1994 1.93(1.35~2.45)* 1994—1999 -0.53(-1.03~-0.02) 1999—2019 -1.83(-1.89~-1.78)* 1990—2019 -1.16(-1.25~-0.90)* DALY率 1990—1994 1.95(1.45~2.43)* 1994—1999 -0.56(-1.04~0.05) 1999—2019 -1.82(-1.87~-1.78)* 1990—2019 -1.16(-1.24~-0.93)* 注:*P<0.05。
下载: 导出CSV
表 4 ADHD发病率和患病率灰色模型拟合结果/10-5
Table 4. Grey model fitting results of incidence and prevalence rate of ADHD/10-5
年份 发病率 患病率 标化发病率 标化患病率 原始值 预测值 相对误差 原始值 预测值 相对误差 原始值 预测值 相对误差 原始值 预测值 相对误差 1990 96.86 96.86 0 2 071.19 2 071.19 0 102.57 102.57 0 1 906.92 1 906.92 0 1991 102.75 114.60 11.53 2 119.33 2 328.65 9.87 108.65 119.77 10.23 1 973.43 2 087.02 10.23 1992 108.15 112.08 3.63 2 162.59 2 296.92 6.21 114.15 120.22 5.31 2 032.57 2 086.58 5.31 1993 112.46 109.61 2.52 2 197.98 2 265.63 3.07 118.73 120.67 1.63 2 080.95 2 086.15 1.63 1994 114.98 107.20 6.76 2 221.32 2 234.77 0.60 122.05 121.12 0.76 2 115.14 2 085.71 0.76 1995 115.00 104.85 8.82 2 229.13 2 204.33 1.11 123.78 121.57 1.79 2 131.59 2 085.27 1.79 1996 112.53 102.54 8.87 2 223.52 2 174.30 2.21 124.40 122.02 1.91 2 133.98 2 084.84 1.91 1997 108.50 100.29 7.56 2 211.71 2 144.68 3.03 124.64 122.48 1.74 2 130.06 2 084.40 1.74 1998 103.43 98.08 5.16 2 194.78 2 115.46 3.61 124.66 122.94 1.38 2 122.16 2 083.96 1.38 1999 97.95 95.92 2.06 2 173.49 2 086.64 3.99 124.60 123.40 0.96 2 112.62 2 083.53 0.96 2000 92.73 93.81 1.17 2 149.48 2 058.22 4.24 124.60 123.86 0.59 2 103.88 2 083.09 0.59 2001 88.32 91.75 3.88 2 117.06 2 030.18 4.10 124.77 124.32 0.36 2 092.78 2 082.66 0.36 2002 84.61 89.73 6.06 2 074.99 2 002.52 3.49 125.13 124.79 0.28 2 077.47 2 082.22 0.28 2003 81.47 87.76 7.72 2 028.63 1 975.24 2.63 125.66 125.25 0.32 2 062.19 2 081.78 0.32 2004 78.88 85.83 8.81 1 983.24 1 948.33 1.70 126.33 125.72 0.48 2 051.10 2 081.35 0.48 2005 76.82 83.94 9.27 1 944.89 1 921.79 1.18 127.11 126.19 0.72 2 048.34 2 080.91 0.72 2006 75.49 82.10 8.76 1 914.58 1 895.61 0.99 128.30 126.66 1.28 2 055.67 2 080.48 1.28 2007 74.79 80.29 7.35 1 888.16 1 869.79 0.97 129.94 127.14 2.16 2 069.37 2 080.04 2.16 2008 74.44 78.53 5.49 1 862.53 1 844.32 0.97 131.63 127.61 3.05 2 085.08 2 079.61 3.05 2009 74.13 76.80 3.60 1 835.05 1 819.19 0.86 132.96 128.09 3.66 2 098.42 2 079.17 3.66 2010 73.54 75.11 2.13 1 804.41 1 794.41 0.55 133.52 128.57 3.71 2 104.92 2 078.73 3.71 2011 72.38 73.46 1.49 1 768.58 1 769.96 0.07 133.12 129.05 3.05 2 101.49 2 078.30 3.05 2012 70.93 71.84 1.29 1 729.23 1 745.85 0.96 132.04 129.53 1.90 2 091.06 2 077.86 1.90 2013 69.68 70.26 0.84 1 690.17 1 722.07 1.88 130.67 130.02 0.50 2 078.05 2 077.43 0.50 2014 68.78 68.72 0.09 1 654.77 1 698.61 2.64 129.42 130.50 0.84 2 066.79 2 076.99 0.84 2015 68.14 67.21 1.35 1 624.09 1 675.47 3.16 128.66 130.99 1.81 2 061.59 2 076.56 1.81 2016 68.10 65.73 3.47 1 598.02 1 652.65 3.41 128.34 131.48 2.45 2 062.64 2 076.12 2.45 2017 68.99 64.28 6.81 1 577.04 1 630.13 3.36 128.12 131.97 3.01 2 064.94 2 075.69 3.01 2018 69.98 62.87 10.16 1 560.50 1 607.93 3.03 127.85 132.47 3.00 2 067.41 2 075.25 3.61 2019 70.41 61.49 12.66 1 546.15 1 586.02 2.57 127.47 132.96 4.31 2 070.84 2 074.82 4.31
下载: 导出CSV
-
[1] POSNER J, POLANCZYK G V, SONUGA B E. Attentio-deficit hyperactivity disorder[J]. Lancet, 2020, 395(10222): 450-462. doi: 10.1016/S0140-6736(19)33004-1 [2] SIBLEY M H, ROHDE L A, SWANSON J M, et al. Late-onset ADHD reconsidered with comprehensive repeated assessments between ages 10 and 25[J]. Am J Psychiatry, 2018, 175(2): 140-149. doi: 10.1176/appi.ajp.2017.17030298 [3] JIN G, ZOU M, ZHANG Y, et al. Time trends, associations and global burden of intraocular foreign bodies[J]. Br J Ophthalmol, 2022, 106(3): 435-439. doi: 10.1136/bjophthalmol-2020-317063 [4] Global Burden of Disease Study 2019. Global burden of 369 diseases and injuries in 204 countries and territories, 1990-2019: a systematic analysis for the Global Burden of Disease Study 2019[J]. Lancet, 2020, 396(10258): 1204-1222. doi: 10.1016/S0140-6736(20)30925-9 [5] MURRAY C J L. The global burden of disease study at 30 years[J]. Nat Med, 2022, 28(10): 2019-2026. doi: 10.1038/s41591-022-01990-1 [6] AKHTAR S, Al-ABKALl J, ALROUGHANI R. Joinpoint regression analysis of trends in multiple sclerosis incidence in Kuwait: 1980-2019[J]. Neuroepidemiology, 2020, 54(6): 472-481. doi: 10.1159/000511205 [7] YANG X, ZOU J, KONG D, et al. The analysis of GM (1, 1) grey model to predict the incidence trend of typhoid and paratyphoid fevers in Wuhan City, China[J]. Medicine (Baltimore), 2018, 97(34): e11787. doi: 10.1097/MD.0000000000011787 [8] SONG P, ZHA M, YANG Q, et al. The prevalence of adult attention-deficit hyperactivity disorder: a global systematic review and Meta-analysis[J]. J Glob Health, 2021, 11: 04009. doi: 10.7189/jogh.11.04009 [9] RAJAPRAKASH M, LEPPERT M L. Attention-deficit/hyperactivity disorder[J]. Pediatr Rev, 2022, 43(3): 135-147. doi: 10.1542/pir.2020-000612 [10] FRATICELLI S, CARATELLI G, BERARDIS D D, et al. Gender differences in attention deficit hyperactivity disorder: an update of the current evidence[J]. Riv Psichiatr, 2022, 57(4): 159-164. [11] GBD 2019 Mental Disorders Collaborators. Global, regional, and national burden of 12 mental disorders in 204 countries and territories, 1990-2019: a systematic analysis for the Global Burden of Disease Study 2019[J]. Lancet Psychiatry, 2022, 9(2): 137-150. doi: 10.1016/S2215-0366(21)00395-3 [12] 翟豪强, 沈德新, 吴秋艳, 等. 针灸治疗儿童注意缺陷多动障碍疗效Meta分析[J]. 临床心身疾病杂志, 2022, 28(5): 93-98. https://www.cnki.com.cn/Article/CJFDTOTAL-LCSX202205020.htmZHAI H Q, SHEN D X, WU Q Y, et al. Meta-analysis of the efficacy of acupuncture in treating children with attention deficit hyperactivity disorder[J]. J Clin Psychosom Dis, 2022, 28(5): 93-98. (in Chinese) https://www.cnki.com.cn/Article/CJFDTOTAL-LCSX202205020.htm [13] GOLMIRZAEI J, MAHBOOBI H, YAZDANPARAST M, et al. Psychopharmacology of attention-deficit hyperactivity disorder: effects and side effects[J]. Curr Pharm Des, 2016, 22(5): 590-594. doi: 10.2174/1381612822666151124235816 [14] CHILDRESS A C, STARK J G. Diagnosis and treatment of attention-deficit/hyperactivity disorder in preschool-aged children[J]. J Child Adolesc Psychopharmacol, 2018, 28(9): 606-614. doi: 10.1089/cap.2018.0057 [15] XU G, STRATHEARN L, LIU B, et al. Twenty-year trends in diagnosed attention-deficit/hyperactivity disorder among US children and adolescents, 1997-2016[J]. JAMA Netw Open, 2018, 1(4): e181471. doi: 10.1001/jamanetworkopen.2018.1471 [16] 孙洁. 促进全民医学科普教育强力推动《"健康中国2030"规划纲要》实施[J]. 中国科技产业, 2018(5): 22-23. https://www.cnki.com.cn/Article/CJFDTOTAL-KJCY201805013.htmSUN J. Promoting universal medical science education strongly promotes the implementation of the "Healthy China 2030" Outline[J]. Chin Sci Technolind, 2018(5): 22-23. (in Chinese) https://www.cnki.com.cn/Article/CJFDTOTAL-KJCY201805013.htm [17] 宋宇尘. 安神定志灵调控注意缺陷多动障碍神经炎症的机制研究[D]. 南京: 南京中医药大学, 2021.SONG Y C. Mechanism of An Shen Ding Zhi Ling in regulating neuroinflammation of attention deficit hyperactivity disorder[D]. Nanjin: Nanjing University of Chinese Medicine, 2021. (in Chinese) -

 点击查看大图
点击查看大图
计量
- 文章访问数: 1232
- HTML全文浏览量: 207
- PDF下载量: 141
- 被引次数: 0