


Routine blood test results of Tibetan children and adolescents in plateau areas
-
摘要:
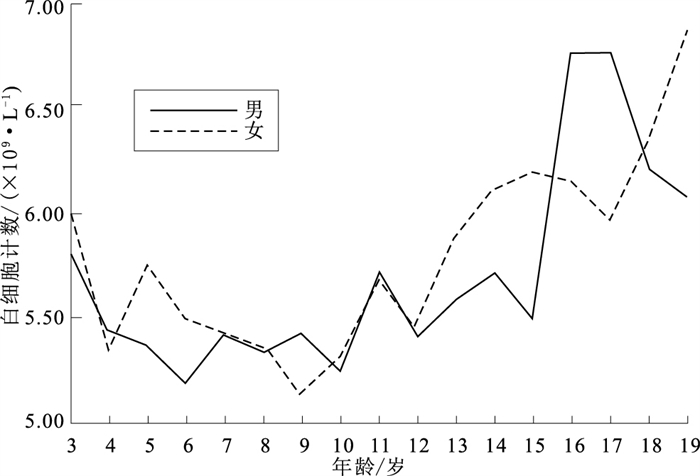
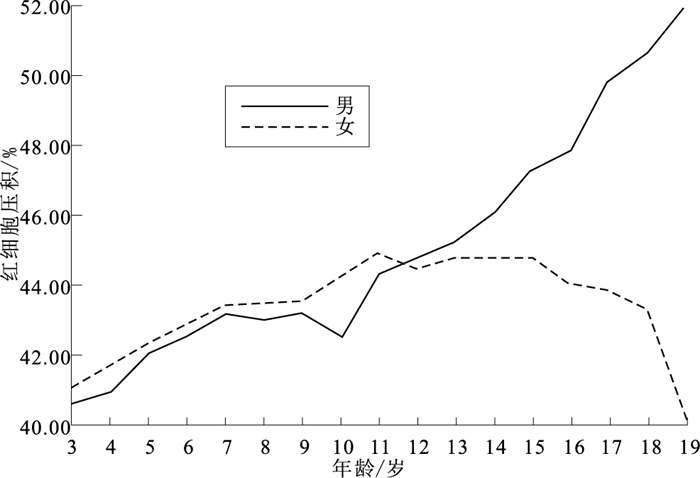
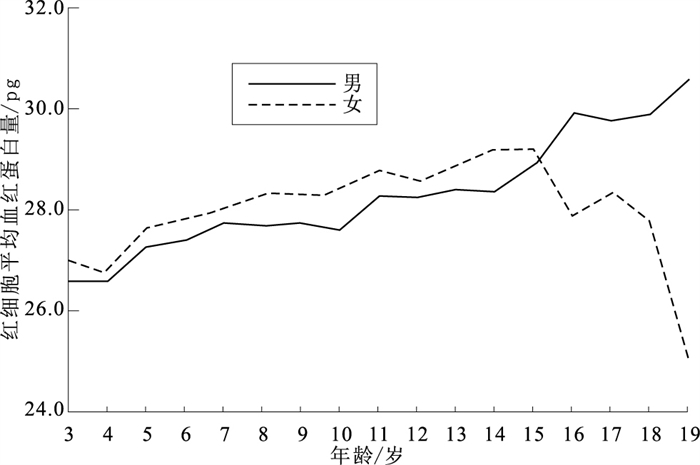
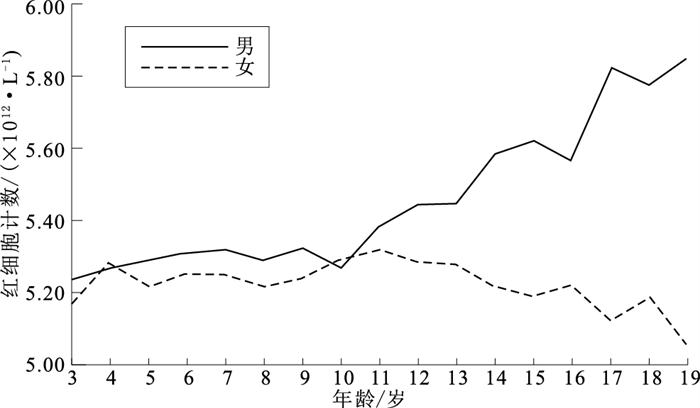
目的 探讨3~19岁高原世居藏族儿童青少年血常规指标水平及其变化趋势,为建立该人群血常规参考值范围提供依据。 方法 采取整群随机抽样方法,以西藏日喀则地区1 568名3~19岁高原世居藏族儿童青少年为研究对象,进行血常规检测,比较各年龄组、不同性别人群血常规指标水平并分析其随年龄变化趋势。 结果 红细胞计数(RBC)、血红蛋白质量浓度(HGB)、红细胞压积(HCT)、平均红细胞体积(MCV)、红细胞平均血红蛋白含量(MCH)、白细胞计数(WBC)、中性粒细胞计数(NEU)、中性粒细胞计数百分比(NEU%)、淋巴细胞数(LYM)、淋巴细胞数百分比(LYM%)、单核细胞计数比例(MON%)、嗜酸性粒细胞计数比例(EOS%)、嗜碱性粒细胞计数比例(BAS%)、血小板计数(PLT)在3~5,6~12,13~15,16~19岁4个年龄段间差异均有统计学意义(F/H值分别为60.22,179.41,249.45,115.03,74.90,14.34,33.46,78.90,49.20,97.29,24.45,24.28,42.65,20.10,P值均 < 0.05),其中RBC、HGB、HCT、MCH红细胞指标在藏族男生中随年龄呈现上升趋势(F值分别为148.77,493.04,623.14,249.92,P值均 < 0.05),在女生中无显著变化趋势(F值分别为1.37,0.15,2.94,0.11,P值均>0.05)。HCT在3~5,6~12,13~15,16~19岁年龄段的男女生间[(41.33±2.31)%,(41.98±2.40)%;(43.28±2.60)%,(43.75±2.36)%;(46.20±3.11)%,(44.83±2.67)%;(51.10±4.15)%,(43.61±4.70)%]差异均有统计学意义(t值分别为-2.10,-2.88,3.50,10.82,P值均 < 0.05)。WBC、NEU、NEU%、LYM、LYM%、单核细胞计数(MON)、MON%等指标在男女中随年龄具有相同的变化趋势(P值均 < 0.05)。从12~13岁开始,RBC、HGB、HCT在高原世居藏族男性与女性青少年中呈现相反的变化趋势并逐渐拉开差距。 结论 红细胞指标在不同年龄、性别的高原世居藏族儿童青少年中变化趋势差异显著,在制定血常规参考值范围时应考虑地域民族、年龄、性别等因素影响。 Abstract:Objective To investigate routine blood test results and secular changes among Tibetan children and adolescents aged from 3 to 19 in the plateau, and to provide the basis for reference range of routine blood test for this population. Methods A total of 1 568 Tibetan children and adolescents aged from 3 to 19 living in Shigatse, Tibet were selected by cluster random sampling method. Routine blood test results and its secular trends were compared by age and gender. Results Significantly differences were found in red blood cell(RBC), hemoglobin(HGB), hematocrit (HCT), mean corpuscular volume (MCV), mean corpuscular hemoglobin(MCH), white blood cell(WBC), neutrophil(NEU), neutrophil percentage (NEU%), lymphocyte(LYM), lymphocyte percentage(LYM%), monocyte percentage(MON%), eosinophil percentage(EOS%), basophil percentage(BAS%) and platelet(PLT) among the four age groups of 3-5, 6-12, 13-15, and 16-19 years (F/H=60.22, 179.41, 249.45, 115.03, 74.90, 14.33, 33.46, 78.90, 49.20, 97.29, 24.45, 24.28, 42.65, 20.10, P < 0.05). Among red blood cell indexes, RBC, HGB, HCT, MCH increased with age in boys(F=148.77, 493.04, 623.14, 249.92, P < 0.05), but there was no similar trend in girls(F=1.37, 0.15, 2.94, 0.11, P>0.05). HCT showed significant sex differences among the four age groups of 3-5 years, 6-12 years, 13-15 years, and 16-19 years [(41.33±2.31)% vs (41.98±2.40)%; (43.28±2.60)% vs (43.75±2.36)%; (46.20±3.11)% vs (44.83±2.67)%; (51.10±4.15)% vs (43.61±4.70)%, t=-2.10, -2.88, 3.50, 10.82, P < 0.05]. WBC, NEU, NEU%, LYM, LYM%, monocyte(MON), and MON% increased significantly with age in both boys and girls (P < 0.05). From the age of 12 to 13, RBC, HGB and HCT in Tibetan male and female adolescents showed an opposite trend and widened gradually. Conclusion Red blood cell index shows significantly different trends among Tibetan adolescents and children of different ages and genders. Regional nationality, age, gender, and other factors should be considered when developing the reference value range of blood routine index. -
Key words:
- Blood /
- Health surveys /
- Analysis of variance /
- Child /
- Adolescent /
- Minority groups
1) 利益冲突声明 所有作者声明无利益冲突。 -

图 1 高原世居藏族男女生红细胞计数年龄变化趋势
Figure 1. The trend of red blood cell with age among native Tibetan boys and girls on the plateau

图 2 高原世居藏族男女生白细胞计数年龄变化趋势
Figure 2. The trend of white blood cell with age among native Tibetan boys and girls on the plateau

图 3 高原世居藏族男女生血小板计数年龄变化趋势
Figure 3. The trend of Platelets with age among native Tibetan boys and girls on the plateau

图 4 高原世居藏族男女生血红蛋白质量浓度年龄变化趋势
Figure 4. The trend of hemoglobin with age among native Tibetan boys and girls on the plateau

图 5 高原世居藏族男女生红细胞压积年龄变化趋势
Figure 5. The trend of hematocrit with age among native Tibetan boys and girls on the plateau

图 6 高原世居藏族男女生红细胞平均血红蛋白量年龄变化趋势
Figure 6. The trend of mean corpuscular hemoglobin with age among native Tibetan boys and girls on the plateau
表 1 不同年龄段藏族儿童青少年血常规指标水平比较(x±s)
Table 1. Comparison of blood routine indexes among Tibetan children and adolescents of different age groups(x±s)
年龄组/岁 人数 RBC/(×1012·L-1) HGB/(g·L-1) HCT/% MCV/fL MCH/pg MCHC/(g·L-1) WBC/(×109·L-1) NEU/(×109·L-1) 3~5 232 5.25±0.32 141.86±9.70 41.65±2.37 79.47±4.50 27.07±1.87 340.43±9.45 5.59±1.65 2.49±1.26 6~12 900 5.30±0.31 148.24±9.86a 43.52±2.49a 82.27±3.95a 28.02±1.60a 340.54±9.47 5.40±1.55 2.72±1.23 13~15 240 5.43±0.36ab 155.73±12.49ab 45.66±3.01ab 84.26±5.05ab 28.74±2.14ab 340.82±10.32 5.78±1.97 3.21±1.81ab 16~19 196 5.63±0.49abc 167.37±22.41abc 49.07±5.44abc 87.08±5.85abc 29.65±2.69abc 340.03±15.18 6.21±1.61ab 3.61±1.48ab F值 60.22 179.41 249.45 115.03 74.90 0.21 14.34 33.46 P值 < 0.01 < 0.01 < 0.01 < 0.01 < 0.01 0.89 < 0.01 < 0.01 年龄组/岁 人数 NEU比例/% LYM/(×109·L-1) LYM比例/% MON比例/% EOS比例/%* BAS比例/%* PLT/(×109·L-1) 3~5 232 43.14±10.58 2.62±0.76 48.15±10.66 6.55±2.44 1.60(1.10, 2.28) 0.20(0.20, 0.34) 291.32±69.55 6~12 900 49.03±9.77a 2.21±0.60a 42.17±9.61a 6.74±1.96 1.50(1.00, 2.30) 0.20(0.20, 0.34) 282.26±66.70 13~15 240 53.41±9.75ab 2.05±0.50ab 37.55±9.14ab 7.05±1.84 1.50(1.00, 2.18) 0.20(0.10, 0.30) 274.42±70.82 16~19 196 56.70±10.04abc 2.00±0.51ab 33.42±9.09abc 8.08±2.62abc 1.20(0.70, 1.80) 0.20(0.10, 0.29) 244.73±67.15abc H/F值 78.90 49.20 97.29 24.45 24.28 42.65 20.10 P值 < 0.01 < 0.01 < 0.01 < 0.01 < 0.01 < 0.01 < 0.01 注: * 数据不符合正态分布,用M(P25, P75)描述;经Bonferroni校正后,a与3~5岁组比较,b与6~12岁组比较,c与13~15岁组比较,P < 0.05。  下载: 导出CSV
下载: 导出CSV
表 2 不同年龄组藏族男女童血常规检查结果比较(x±s)
Table 2. Comparison of blood routine examination results between Tibetan boys and girls of different age groups(x±s)
年龄组/岁 性别 人数 统计值 RBC/(×1012·L-1) HGB/(g·L-1) HCT/% MCV/fL MCH/pg MCHC/(g·L-1) WBC/(×109·L-1) NEU/(×109·L-1) 3~5 男 116 5.27±0.33 141.24±9.49 41.33±2.31 78.53±4.15 26.85±1.80 341.59±9.48 5.50±1.50 2.39±1.06 女 116 5.23±0.32 142.48±9.91 41.98±2.40 80.40±4.65 27.30±1.92 339.26±9.31 5.68±1.79 2.59±1.44 t值 0.98 -0.98 -2.10 -3.23 -1.84 1.90 -0.85 -1.23 P值 0.33 0.33 0.04 < 0.01 0.07 0.06 0.40 0.22 6~12 男 442 5.33±0.32 147.95±10.47 43.28±2.60 81.25±3.84 27.78±1.65 341.72±10.02 5.39±1.56 2.70±1.25 女 458 5.26±0.29 148.51±9.24 43.75±2.36 83.24±3.81 28.25±1.53 339.39±8.76 5.41±1.53 2.75±1.20 t值 3.44 -0.85 -2.88 -7.82 -4.51 3.73 -0.21 -0.59 P值 < 0.01 0.40 < 0.01 < 0.01 < 0.01 < 0.01 0.84 0.56 13~15 男 146 5.55±0.35 158.17±12.66 46.20±3.11 83.36±4.97 28.55±2.15 342.18±10.52 5.60±2.02 3.08±1.92 女 94 5.24±0.30 151.95±11.28 44.83±2.67 85.67±4.87 29.04±2.09 338.69±9.67 6.05±1.86 3.41±1.63 t值 7.14 3.88 3.50 -3.55 -1.75 2.59 -1.72 -1.37 P值 < 0.01 < 0.01 < 0.01 < 0.01 0.08 0.01 0.09 0.17 16~19 男 143 5.80±0.42 175.90±16.02 51.10±4.15 88.12±4.81 30.30±1.83 343.97±11.18 6.23±1.67 3.58±1.57 女 53 5.17±0.37 144.34±21.00 43.61±4.70 84.30±7.38 27.89±3.68 329.40±19.12 6.17±1.45 3.70±1.22 t值 9.61 11.22 10.82 3.45 4.58 5.23 0.21 -0.50 P值 < 0.01 < 0.01 < 0.01 < 0.01 < 0.01 < 0.01 0.83 0.62 年龄组/岁 性别 人数 统计值 NEU比例/% LYM/(×109·L-1) LYM比例/% MON比例/% EOS比例/%* BAS比例/%* PLT/(×109·L-1) 3~5 男 116 42.49±9.70 2.61±0.77 48.37±10.06 6.86±2.61 1.80(1.30,2.58) 0.20(0.20,0.40) 294.29±71.80 女 116 43.78±11.40 2.62±0.74 47.93±11.27 6.24±2.24 1.50(0.92,2.10) 0.20(0.20,0.30) 288.35±67.39 Z/t值 -0.93 -0.11 0.32 1.95 2.00 0.85 0.65 P值 0.36 0.91 0.75 0.06 0.05 0.40 0.52 6~12 男 442 48.65±9.68 2.20±0.57 42.13±9.58 1.98±1.59 1.70(1.10,2.40) 0.20(0.20,0.40) 284.97±65.29 女 458 49.41±9.86 2.21±0.62 42.20±9.65 1.66±1.52 1.40(0.90,2.10) 0.20(0.20,0.30) 279.65±68.00 Z/t值 -1.17 -0.38 -0.10 3.06 4.08 1.34 1.20 P值 0.24 0.70 0.92 < 0.01 < 0.01 0.18 0.23 13~15 男 146 52.74±9.82 2.00±0.49 37.77±9.21 7.17±1.98 1.80(1.30, 2.53) 0.20(0.10, 0.30) 269.30±57.68 女 94 54.47±9.59 2.14±0.50 37.19±9.07 6.86±1.59 1.25(0.70, 1.60) 0.20(0.10, 0.24) 282.37±87.16 Z/t值 -1.35 -2.12 0.48 1.35 5.18 1.37 -1.28 P值 0.18 0.04 0.63 0.18 < 0.01 0.17 0.20 16~19 男 143 55.83±10.32 2.03±0.49 34.07±9.28 8.27±2.79 1.20(0.70, 1.80) 0.20(0.10, 0.24) 230.50±54.50 女 53 59.07±8.92 1.91±0.58 31.65±8.37 7.57±2.06 1.30(0.80, 1.75) 0.20(0.10, 0.30) 283.15±82.07 Z/t值 -2.03 1.53 1.67 1.68 0.71 0.34 -4.33 P值 0.04 0.13 0.10 0.10 0.48 0.74 < 0.01 注: * 数据不符合正态分布,用M(P25, P75)描述。
下载: 导出CSV
-
[1] 王红. 血常规检测的临床意义分析与研究[J]. 青岛医药卫生, 2013, 45(2): 140-141. doi: 10.3969/j.issn.1006-5571.2013.02.028WANG H. Analysis and study on clinical significance of blood routine examination[J]. Qingdao Med J, 2013, 45(2): 140-141. doi: 10.3969/j.issn.1006-5571.2013.02.028 [2] WEI Y, SONG Z, DAN L, et al. Establishment of reference intervals for blood cell analysis of adult Tibetan farmers and herdsmen over 4100 meters above sea level in Tibet based on a health survey[J]. High Alt Med Biol, 2020, 21(3): 223-231. doi: 10.1089/ham.2020.0006 [3] LI C, LI X, LIU J, et al. Investigation of the differences between the Tibetan and Han populations in the hemoglobin-oxygen affinity of red blood cells and in the adaptation to high-altitude environments[J]. Hematology, 2018, 23(5): 309-313. doi: 10.1080/10245332.2017.1396046 [4] 宋佳琪, 马振, 曾泽, 等. 某部长期驻4 500 m高原官兵血常规及血生化检查特点分析[J]. 人民军医, 2021, 64(9): 801-804. doi: 10.3969/j.issn.1000-9736.2021.09.001SONG J Q, MA Z, ZENG Z, et al. Analysis on the characteristics of blood routine and blood biochemical examination of officers and soldiers stationed at 4 500 m plateau for a long time[J]. People's Military Surgeon, 2021, 64(9): 801-804. doi: 10.3969/j.issn.1000-9736.2021.09.001 [5] 国家卫生部. 血细胞分析参考区间: WS/T 405-2012[S]. 北京: 中国标准出版社, 2013.Ministry of Health of the PRC. Reference intervals for blood cell analysis: WS/T 405-2012[S]. Beijing: Standards Press of China, 2013. [6] 国家卫生健康委员会. 儿童血细胞分析参考区间: WS/T 779-2021[S]. 北京: 中国标准出版社, 2021.National Health Commission of the PRC. Reference intervals of blood cell analysis for children: WS/T 779-2021[S]. Beijing: Standards Press of China, 2021. [7] 次仁潘多. 西藏不同海拔高度世居藏族和移居人群高原适应不全的流行病学调查与分子机制研究[D]. 拉萨: 西藏大学, 2017.CIREN P D. Epidemiological investigation and molecular mechanism of altitude maladjustment of native Tibetans and immigrants at different altitudes in Tibet[D]. Lhasa: Tibet University, 2017. [8] TAHMASEBI H, HIGGINS V, BOHN M K, et al. CALIPER hematology reference standards (I)[J]. Am J Clin Pathol, 2020, 154(3): 330-341. doi: 10.1093/ajcp/aqaa059 [9] DING Y, ZHOU L, XIA Y, et al. Reference values for peripheral blood lymphocyte subsets of healthy children in China[J]. J Allergy Clin Immunol, 2018, 142(3): 970-973. doi: 10.1016/j.jaci.2018.04.022 [10] 鲁道远, 张驰. 武汉地区0~12岁健康儿童血常规检验项目参考区间调查[J]. 中国妇幼保健, 2020, 35(11): 2068-2073.LU D Y, ZHANG C. Investigation on reference interval of blood routine test items of healthy children aged 0~12 years in Wuhan[J]. Matern Child Health Care China, 2020, 35(11): 2068-2073. [11] ANGELO D, TRAVIS N, KAIQI S, et al. Altitude omics: red blood cell metabolic adaptation to high altitude hypoxia[J]. J Proteom Res, 2016, 15(10): 3883-3895. doi: 10.1021/acs.jproteome.6b00733 [12] REN Q, LV X, YANG L, et al. Erythrocytosis and performance of HbA1c in detecting diabetes on an oxygen-deficient plateau: a population-based stud[J]. J Clin Endocrinol Metab, 2020, 105(4): dgaa001. [13] LUO X, FENG L, BAI X J, et al. Continuous changes in biological levels of complete blood count in a high altitude area of China[J]. SAGE Open Med, 2020, 8: 1-7. [14] GASSMMAN M, MAIRBAURL H, LIVSHITS L, et al. The increase in hemoglobin concentration with altitude varies among human populations[J]. Ann N Y Acad Sci, 2019, 1450(1): 204-220. [15] 谢慎威, 陈波, 刘秉林, 等. 不同海拔高原习服汉族与世居藏族的血常规比较研究[J]. 西南国防医药, 2019, 29(7): 781-783. doi: 10.3969/j.issn.1004-0188.2019.07.021XIE S W, CHEN B, LIU B L, et al. Comparison of the routine blood indexes between acclimatized Han population and native Tibetan at different high altitudes[J]. Med J Natl Defend Forces Southwest China, 2019, 29(7): 781-783. doi: 10.3969/j.issn.1004-0188.2019.07.021 [16] 高原, 邹琛, 蒋婕, 等. 上海市526例1~12岁儿童静脉血血常规正常参考区间建立[J]. 国际检验医学杂志, 2015, 36(16): 2332-2334. doi: 10.3969/j.issn.1673-4130.2015.16.017GAO Y, ZOU C, JIANG J, et al. Determination of normal reference ranges for venous blood count among 526 children aging from 1 year old to 12 years old in Shanghai[J]. Int Lab Med, 2015, 36(16): 2332-2334. doi: 10.3969/j.issn.1673-4130.2015.16.017 [17] 李秀娟, 张炎胜, 蔡建兴. 厦门地区8 492名儿童末梢血血细胞参数参考区间的建立[J]. 检验医学, 2017, 32(6): 504-507. doi: 10.3969/j.issn.1673-8640.2017.06.013LI X J, ZHANG Y S, CAI J X. Establishment of reference interval for peripheral blood cell parameters of 8492 children in Xiamen[J]. Lab Med, 2017, 32(6): 504-507. doi: 10.3969/j.issn.1673-8640.2017.06.013 [18] 肖军, 李小薇, 雷慧芬, 等. 高原环境对人外周血细胞的影响[J]. 中国输血杂志, 2017, 30(8): 870-872.XIAO J, LI X W, LEI H F, et al. Effects of high altitude environment on human peripheral blood cells[J]. Chin J Blood Transfus, 2017, 30(8): 870-872. [19] KHANNA K, MISHRA K P, GANJU L, et al. High-altitude-induced alterations in gut-immune axis: a review[J]. Int Rev Immunol, 2018, 37(2): 119-126. doi: 10.1080/08830185.2017.1407763 [20] BACHMAN E, TRAVISION T G, BASARIA S, et al. Testosterone induces erythrocytosis via increased erythropoietin and suppressed hepcidin: evidence for a new erythropoietin/hemoglobin set point[J]. J Gerontol A Biol Sci Med Sci, 2014, 69(6): 725-735. doi: 10.1093/gerona/glt154 [21] SANDEEP D, HUSAM G, MANAV B, et al. Effect of testosterone on hepcidin, ferroportin, ferritin and iron binding capacity in patients with hypogonadotropic hypogonadism and type 2 diabetes[J]. Clin Endocrinol(Oxf), 2016, 85(5): 772-780. doi: 10.1111/cen.13130 [22] GONZALES G F. Hemoglobin and testosterone: importance on high altitude acclimatization and adaptation[J]. Rev Peru Med Exp Salud Public, 2011, 28(1): 92-100. doi: 10.1590/S1726-46342011000100015 [23] NGUYEN L, WANG Z, CHOWDHURY A Y, et al. Functional compensation between hematopoietic stem cell clones in vivo[J]. Embo Rep, 2018, 19(8): e45702. [24] KIERS D, TUNJUNGPUTRI R N, BORKUS R, et al. The influence of hypoxia on platelet function and plasmatic coagulation during systemic inflammation in humans in vivo[J]. Platelets, 2019, 30(7): 927-930. doi: 10.1080/09537104.2018.1557617 -



 点击查看大图
点击查看大图
计量
- 文章访问数: 437
- HTML全文浏览量: 190
- PDF下载量: 25
- 被引次数: 0