


Trends and risk factors of anaemia among the nutrition improvement program for rural compulsory education students aged 6-15 years, Hunan Province
-
摘要:
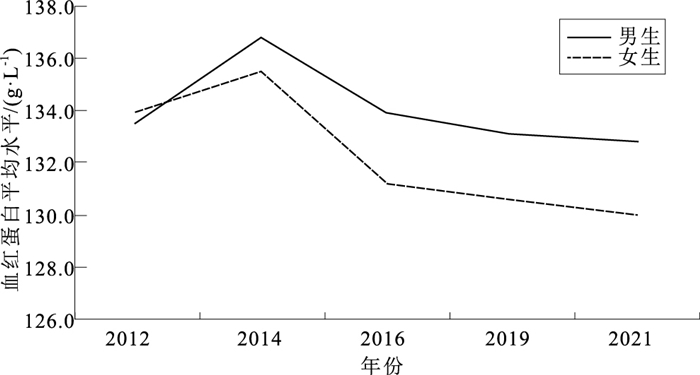
目的 了解湖南省2012—2021年“农村义务教育学生营养改善计划”实施地区6~15岁学生贫血的流行规律及影响因素,为更好地实施营养改善计划提供支撑和建议。 方法 采用整群随机抽样的方法,在湖南省实施营养改善计划以及开展重点监测的县抽取义务教育学生,进行身高、体重、血红蛋白、饮食习惯、健康知识知晓情况的调查。 结果 湖南省从2012年实施营养改善计划以来,贫血率从12.8%下降到9.3%;血红蛋白平均体积浓度从133.9 g/L下降到130.0 g/L;每天保证吃肉的学生、每次能吃到3个乒乓球大小肉量的学生分别从20.4%,21.4%逐年递增到47.3%,47.3%;每天能吃3种以上蔬菜的学生除2016和2019年达到39.1%和32.6%,其他年份均未超过30%;每次能吃够3个乒乓球及以上蔬菜量的学生从19.5%递增到39.6%;每天不吃零食的学生从13.1%增加到76.9%;每天不喝饮料的学生从36.5%增加到90.7%。女生、12岁及以上学生、不能保证每天都吃肉、每次吃肉量不足1个乒乓球、每次吃蔬菜以及水果的量不足3个乒乓球、每天吃蔬菜种类少于3种的学生、生长发育迟缓的学生更容易发生贫血,且各年份学生贫血发生的影响因素有所不同。 结论 农村义务教育学生营养改善计划的实施在一定程度上改善了湖南农村地区义务教育阶段学生的营养状况,然而贫血现象依然存在。应不断提升学生健康素养,有针对性地开展科学合理膳食的分类指导和干预。 Abstract:Objective To investigate the prevalence of anemia among students aged 6-15 years old participated in the Nutrition Improvement Program for Rural Compulsory Education Program in 2012-2021 in Hunan Province, and to explore associated factors. Methods A cluster random sampling method was used. The survey was conducted among compulsory education students who came from counties in Hunan Province where nutrition improvement plan and key surveillance were carried out. Height and weight were measured, hemoglobin, dietary habits and health knowledge were collected. Results Since the implementation of nutrition improvement plan in 2012, the anemia rate decreased from 12.8% to 9.3%, the average hemoglobin content decreased from 133.9 g/L to 130.0 g/L. The proportion of students eating meat every day increased from 20.4% to 47.3%. Students eating three or more servings of table tennis ball-size of meal increased from 21.4% to 47.3%. The proportion of students eating more than three kinds of vegetables per day was 39.1% in 2016 and 32.6% in 2019, and less than 30% in other years. The proportion of students eating three or more servings of table tennis ball-size of vegetables increased from 19.5% to 39.6%, and the proportion of students eating snack less than once a day increased from 13.1% to 76.9%. The proportion of students drinking beverages less than once a day increased from 36.5% to 90.7%. Girls, older than 12 years, not eating meat every day, and who eat less than 1 serving of table tennis ball-size of meat, eat less than 3 servings of table tennis ball-size of vegetables and fruit at one time, and who eat less than 3 kinds of vegetables every day, and those who grow slowly had higher risk of anemia. Potential factors of anemia in students varied by survey year. Conclusion The implementation of the compulsory education has improved the nutritional status of compulsory education students in rural areas of Hunan Province, but anemia still occurs. Potential factors associated with childhood anemia are changing. Child health literacy education should adapt to the changing social and economic enviornment, as well as lifestyles. Targeted and appropriate nutritional education and intervention are greatly needed. -
Key words:
- Nutrition policy /
- Anemia /
- Regression analysis /
- Students /
- Rural population
1) 利益冲突声明 所有作者声明无利益冲突。 -

图 1 2012—2021年学生血红蛋白平均水平
Figure 1. Average hemoglobin content of the students from year 2012-2021

图 2 2012—2021年学生贫血发生率
Figure 2. Anaemia prevalence trends of the students from year 2012-2021
表 1 营养改善计划地区是否贫血学生营养状况分布比较
Table 1. Coparison of nutritional status distribution among students with and without anemia in the rural nutrition improvement program area
年份 是否贫血 人数 正常 超重 肥胖 生长迟缓 消瘦 χ2值 P值 2012 贫血 263 190(72.2) 17(6.5) 13(4.9) 2(0.8) 41(15.6) 5.36 0.25 正常 1 788 1 304(72.9) 160(8.9) 68(3.8) 31(1.7) 225(12.6) 小计 2 051 1 494(72.8) 177(8.6) 81(3.9) 33(1.6) 266(13.0) 2014 贫血 286 219(76.6) 13(4.5) 10(3.5) 5(1.7) 39(13.6) 8.59 0.07 正常 2 828 2 138(75.6) 246(8.7) 107(3.8) 28(1.0) 309(10.9) 小计 3 114 2 357(75.7) 259(8.3) 117(3.8) 33(1.1) 348(11.2) 2016 贫血 72 198(72.8) 24(8.8) 12(4.4) 7(2.6) 31(11.4) 7.74 0.10 正常 3 071 2 229(72.6) 339(11.0) 132(4.3) 28(0.9) 343(11.2) 小计 3 343 2 427(72.6) 363(10.9) 144(4.3) 35(1.0) 374(11.2) 2019 贫血 345 250(72.5) 22(6.4) 11(3.2) 4(1.2) 58(16.8) 19.16 < 0.01 正常 3 071 2 269(73.9) 256(8.3) 197(6.4) 14(0.5) 335(10.9) 小计 3 416 2 519(73.7) 278(8.1) 208(6.1) 18(0.5) 393(11.5) 2021 贫血 418 288(68.9) 38(9.1) 56(13.4) 11(2.6) 25(6.0) 9.80 0.04 正常 4 049 2 724(66.9) 463(11.4) 618(15.2) 46(1.1) 218(5.4) 小计 4 481 3 012(67.1) 501(11.2) 674(15.0) 57(1.3) 243(5.4) 合计 贫血 1 584 1 145(72.3) 114(7.2) 102(6.4) 29(1.8) 194(12.2) 32.33 < 0.01 正常 14 827 10 664(71.9) 1 464(9.9) 1 122(7.6) 147(1.0) 1 430(9.6) 小计 16 411 11 809(72.0) 1 578(9.6) 1 224(7.5) 176(1.1) 1 624(9.9) 注:()内数字为构成比/%。  下载: 导出CSV
下载: 导出CSV
表 2 农村营养改善计划地区学生饮食习惯分布2012—2021年间比较
Table 2. Coparison of the distribution of students' dietary habits in the rural nutrition improvement program area from year 2012-2021
饮食习惯 选项 2012年
(n=1 272)2014年
(n=2 168)2016年
(n=2 072)2019年
(n=1 910)2021年
(n=3 349)χ趋势2值 P值 每周吃肉情况 每天吃 260(20.4) 311(14.3) 508(24.5) 761(39.8) 1 585(47.3) 755.00 < 0.01 未能每天吃 894(70.3) 1 683(77.6) 1 471(71.0) 1 051(55.0) 1 712(51.1) 433.19 < 0.01 基本不吃 118(9.3) 174(8.0) 93(4.5) 98(5.1) 52(1.6) 161.45 < 0.01 每次吃肉量 ≥3个乒乓球 139(10.9) 290(13.4) 323(15.6) 362(19.0) 1 189(35.5) 504.17 < 0.01 1~ < 3个乒乓球 905(71.1) 1 566(72.2) 1 472(71.0) 1 345(70.4) 1 637(48.9) 327.87 < 0.01 < 1个乒乓球 228(17.9) 312(14.4) 277(13.4) 203(10.6) 523(15.6) 2.29 0.13 每天吃蔬菜种类 ≥3种 325(25.6) 415(19.1) 811(39.1) 622(32.6) 529(15.8) 33.03 < 0.01 < 3种 879(69.1) 1 578(72.8) 1 218(58.8) 1 225(64.1) 2 682(80.1) 59.11 < 0.01 基本不吃 68(5.3) 175(8.1) 43(2.1) 63(3.3) 138(4.1) 24.04 < 0.01 每次吃蔬菜量 ≥3个乒乓球 248(19.5) 454(20.9) 444(21.4) 986(51.6) 1 325(39.6) 446.99 < 0.01 1~ < 3个乒乓球 925(72.7) 1 535(70.8) 1 492(72.0) 776(40.6) 1 536(45.9) 631.31 < 0.01 < 1个乒乓球 99(7.8) 179(8.3) 136(6.6) 148(7.7) 488(14.6) 72.45 < 0.01 每周吃水果情况 每天吃 191(9.2) 361(18.9) 753(22.5) 147.23 < 0.01 未能每天吃 1 441(69.5) 1 386(72.6) 2 465(73.6) 10.00 < 0.01 基本不吃 440(21.2) 163(8.5) 131(3.9) 407.34 < 0.01 每次吃水果量 ≥3个乒乓球 323(15.6) 1 082(56.6) 1 573(47.0) 426.39 < 0.01 1~ < 3个乒乓球 1 532(73.9) 686(35.9) 1 502(44.8) 353.72 < 0.01 < 1个乒乓球 217(10.5) 142(7.4) 274(8.2) 6.92 0.01 每天吃零食情况 < 1次 166(13.1) 1 176(56.8) 1 210(63.4) 2 576(76.9) 1 337.35 < 0.01 1次 380(29.9) 512(24.7) 347(18.2) 603(18.0) 91.06 < 0.01 ≥2次 726(57.1) 384(18.5) 353(18.5) 170(5.1) 1 279.93 < 0.01 每天喝饮料情况 < 1次 464(36.5) 1 143(55.2) 1 580(82.7) 3 037(90.7) 1 716.08 < 0.01 1次 536(42.1) 560(27.0) 236(12.4) 270(8.1) 810.54 < 0.01 ≥2次 272(21.4) 369(17.8) 94(4.9) 42(1.3) 674.84 < 0.01 注:()内数字为构成比/%,2012,2014年未开展吃水果调查,2014年未开展吃水果、吃零食、喝饮料调查。
下载: 导出CSV
表 3 农村营养改善计划地区学生2012年贫血发生因素Logistic回归分析[OR值(OR值95%CI)]
Table 3. Logistic regression analysis on the incidence of anemia among students in rural areas in 2012[OR(OR95%CI)]
自变量 选项 男生(n=645) 女生(n=627) 每次吃肉量 ≥3个乒乓球 1.00 1.00 < 1个乒乓球 2.32(0.83~6.52) 8.18(1.75~38.14)** 1~ < 3个乒乓球 1.62(0.64~4.12) 4.18(0.95~18.50) 每天吃蔬菜种类 ≥3种 1.00 1.00 基本不吃 1.80(0.60~5.36) 5.00(1.63~15.35)** < 3种 1.32(0.71~2.44) 2.37(1.08~5.21)* 注:*P < 0.05,**P < 0.01。
下载: 导出CSV
表 4 农村营养改善计划地区学生2014年贫血发生因素Logistic回归分析[OR值(OR值95%CI)]
Table 4. Logistic regression analysis on the incidence of anemia among students in rural areas in 2014[OR(OR95%CI)]
自变量 选项 男生(n=1 105) 女生(n=1 063) 每周吃肉情况 每天吃 1.00 1.00 基本不吃 0.71(0.22~2.31) 0.66(0.26~1.63) 未能每天吃 1.13(0.49~2.63) 0.50(0.26~1.00)* 每次吃肉量 ≥3个乒乓球 1.00 1.00 < 1个乒乓球 3.80(1.18~12.28)* 3.96(1.34~11.72)* 1~ < 3个乒乓球 3.18(1.09~9.31)* 2.32(0.67~7.98) 蛋白质良好来源 知晓 1.00 1.00 不知晓 3.05(1.47~6.31)** 2.00(1.12~3.57)* 如何预防缺铁性贫血 知晓 1.00 1.00 不知晓 1.12(0.63~2.01) 2.52(1.38~4.61)* 注:*P < 0.05,**P < 0.01。
下载: 导出CSV
表 5 农村营养改善计划地区学生2016年贫血发生因素Logistic回归分析[OR值(OR值95%CI)]
Table 5. Logistic regression analysis on the incidence of anemia among students in rural areas in 2016[OR(OR95%CI)]
自变量 选项 男生(n=1 050) 女生(n=1 022) 年龄/岁 ≥15 1.00 1.00 < 12 0.42(0.11~1.64) 0.20(0.06~0.66)** 12~ < 15 0.47(0.13~1.76) 0.35(0.11~1.15) 每次吃肉量 ≥3个乒乓球 1.00 1.00 < 1个乒乓球 71.97(12.56~412.60)** 68.88(17.71~267.99)** 1~ < 3个乒乓球 3.17(0.59~16.98) 3.08(0.90~10.50) 每次吃蔬菜量 ≥3个乒乓球 1.00 1.00 < 1个乒乓球 6.16(1.54~24.58)* 2.45(0.65~9.21) 1~ < 3个乒乓球 0.35(0.05~2.39) 2.01(0.35~11.50) 每次吃水果量 ≥3个乒乓球 1.00 1.00 < 1个乒乓球 0.16(0.04~0.68)* 0.18(0.05~0.69)* 1~ < 3个乒乓球 0.09(0.02~0.45)** 0.02(0.00~0.13)** 营养水平 正常 1.00 1.00 生长迟缓 10.58(1.01~111.99)* 1.46(0.28~7.58) 消瘦 1.75(0.75~4.09) 0.22(0.04~1.28) 超重肥胖 1.02(0.38~2.76) 0.40(0.15~1.09) 注:*P < 0.05,**P < 0.01。
下载: 导出CSV
表 6 农村营养改善计划地区学生2019年贫血发生因素Logistic回归分析[OR值(OR值95%CI)]
Table 6. Logistic regression analysis on the incidence of anemia among students in rural areas in 2019[OR(OR95%CI)]
自变量 选项 男生(n=969) 女生(n=941) 年龄/岁 ≥15 1.00 1.00 < 12 0.30(0.13~0.67)** 0.44(0.19~0.99)* 12~ < 15 0.33(0.13~0.83)* 0.67(0.29~1.55) 每周吃肉情况 每天吃 1.00 1.00 基本不吃 3.16(1.59~6.29)** 2.06(1.13~3.76)* 未能每天吃 1.21(0.23~6.35) 1.82(0.60~5.57) 注:*P < 0.05,**P < 0.01。
下载: 导出CSV
表 7 农村营养改善计划地区学生2021年贫血发生因素Logistic回归分析[OR值(OR值95%CI)]
Table 7. Logistic regression analysis on the incidence of anemia among students in rural areas in 2021[OR(OR95%CI)]
自变量 选项 男生(n=1 692) 女生(n=1 657) 年龄/岁 ≥15 1.00 1.00 < 12 0.25(0.06~1.16) 3.20(0.86~11.82) 12~ < 15 0.55(0.23~1.32) 2.99(1.40~6.42)** 营养水平 正常 1.00 1.00 生长迟缓 4.57(1.36~15.39)* 1.14(0.14~9.17) 消瘦 1.09(0.56~2.13) 0.68(0.27~1.77) 超重肥胖 0.74(0.49~1.13) 0.76(0.50~1.15) 注:*P < 0.05,**P < 0.01。
下载: 导出CSV
-
[1] 葛均波, 徐永健. 内科学[M]. 9版. 北京: 人民卫生出版社, 2018: 532-544.GE J B, XU Y J. Internal medicine[M]. 9 ed. Beijing: People's Medical Publishing House, 2018: 532-544. [2] 杨锡强, 易著文. 儿科学[M]. 6版. 北京: 人民卫生出版社, 2006: 397.YANG X Q, YI Z W. Pediatrics[M]. 6 ed. Beijing: People's Medical Publishing House, 2006: 397. [3] 世界卫生组织. 血红蛋白浓度用于诊断贫血及评估其严重性[R]. Geneva: WHO, 2011: 1-6.World Health Organization. Hemoglobin concentration is used to diagnose anemia and assess its severity[R]. Geneva: WHO, 2011: 1-6. [4] 中华人民共和国国家卫生和计划生育委员会. 学龄儿童青少年超重与肥胖筛查: WS/T 586—2018[S]. 北京: 中国标准出版社, 2018: 1-3.National Health Commission of the PRC. Screening for overweight and obesity among school-age children and adolescents: WS/T 586-2018[S]. Beijing: Standards Press of China, 2018: 1-3. [5] 中华人民共和国国家卫生和计划生育委员会. 学龄儿童青少年营养不良筛查: WS/T 456—2014[S]. 北京: 中国标准出版社, 2014: 1-4.National Health Commission of the PRC. Screening standard for malnutrition of school-age children and adolescents: WS/T 586-2018[S]. Beijing: Standards Press of China, 2014: 1-4. [6] 沈渝, 许瑾娣. 青少年贫血[J]. 中国学校卫生, 2004, 25(5): 641-642. doi: 10.3969/j.issn.1000-9817.2004.05.089SHEN Y, XU J D. Juvenile anemia[J]. Chin J Sch Health, 2004, 25(5): 641-642. doi: 10.3969/j.issn.1000-9817.2004.05.089 [7] WHO. Worldwide prevalence of anaemia 1993-2005[R]. Geneva: World Health Organization, 2008: 7-8. [8] 张洋. 儿童青少年缺铁性贫血防治研究进展[J]. 中国处方药, 2020, 18(3): 19-21. doi: 10.3969/j.issn.1671-945X.2020.03.011ZHANG Y. Research progress on prevention and treatment of iron deficiency anemia in children and adolescents[J]. J China Prescrip Drug, 2020, 18(3): 19-21. doi: 10.3969/j.issn.1671-945X.2020.03.011 [9] 高春海, 胡小琪, 张倩, 等. 2016年中国贫困农村地区留守儿童贫血及其相关因素分析[J]. 中华流行病学杂志, 2019(12): 1548-1553. doi: 10.3760/cma.j.issn.0254-6450.2019.12.008GAO C H, HU X Q, ZHANG Q, et al. Anemia status and related factors among left-behind children in poverty-stricken rural areas, in China, 2016[J]. Chin J Epidemiol, 2019, 40(12): 1548-1553. doi: 10.3760/cma.j.issn.0254-6450.2019.12.008 [10] 陈润, 李孙明, 徐可欣. 百色市中小学生贫血检出现状及影响因素研究[J]. 华南预防医学, 2021, 47(12): 1514-1517. https://www.cnki.com.cn/Article/CJFDTOTAL-GDWF202112006.htmCHEN R, LI S M, XU K X. Detection status and related factors of anemia among primary and middle school students in Baise[J]. South Chin J Prev Med, 2021, 47(12): 1514-1517. https://www.cnki.com.cn/Article/CJFDTOTAL-GDWF202112006.htm [11] 崔娜. 12~14岁青春前期青少年学生的缺铁性贫血状况及其影响因素[J]. 中国医药指南, 2017, 15(34): 60-61. https://www.cnki.com.cn/Article/CJFDTOTAL-YYXK201734046.htmCUI N. The iron deficiency anemia and its influencing factors of pre-adolescent students aged from 12 to 14[J]. Guide China Med, 2017, 15(34): 60-61. https://www.cnki.com.cn/Article/CJFDTOTAL-YYXK201734046.htm [12] 陈小剑, 方佩佩, 乔增培, 等. 11~15岁青少年营养性缺铁性贫血的调查[J]. 中国现代医生, 2011, 49(13): 86-89. doi: 10.3969/j.issn.1673-9701.2011.13.047CHEN X J, FANG P P, QIAO Z P, et al. Investigation on nutritional iron deficiency anemia of adolescents aged 11-15[J]. China Modern Doct, 2011, 49(13): 86-89. doi: 10.3969/j.issn.1673-9701.2011.13.047 [13] 孙凯丽, 职心乐, 张欣. 天津市2014年儿童青少年贫血及营养状况[J]. 中国学校卫生, 2016, 37(8): 1127-1129. doi: 10.16835/j.cnki.1000-9817.2016.08.003SUN K L, ZHI X Y, ZHANG X. The prevalence of anemia and its relation with nutritional status among children and adolescents in Tianjin in 2014[J]. Chin J Sch Health, 2016, 37(8): 1127-1129. doi: 10.16835/j.cnki.1000-9817.2016.08.003 [14] 朱艳娜, 富诗岚, 何宝婷, 等. 广州市7~14岁学龄儿童营养状况与贫血相关性分析[J]. 中国热带医学, 2014, 14(11): 1335-1339. https://www.cnki.com.cn/Article/CJFDTOTAL-RDYX201411013.htmZHU Y N, FU S L, HE B T, et al. Relationship between nutritional status and anemia among children aged 7-14 years in Guangzhou City[J]. China Tropic Med, 2014, 14(11): 1335-1339. https://www.cnki.com.cn/Article/CJFDTOTAL-RDYX201411013.htm [15] HESHMAT M KATAYOON B, SIROUSH Z, et al. Increasing prevalence of iron deficiency in overweight and obese children and adolescent (Tehran Adolescent Obesity Study)[J]. Europ J Pediat, 2006, 165(165): 813-814. [16] 陈允伦, 郭红霞. 小儿肥胖与贫血[J]. 职业与健康, 2002, 18(6): 119. doi: 10.3969/j.issn.1004-1257.2002.06.117CHEN Y L, GUO H X. Obesity and anemia in children[J]. Occup Health, 2002, 18(6): 119. doi: 10.3969/j.issn.1004-1257.2002.06.117 [17] 王婷婷. 2012—2014年"农村学生营养改善计划"实施地区学生贫血状况的变化及相关因素的研究[D]. 北京: 中国疾病预防控制中心, 2016.WANG T T. Study on the changes of anemia and its related factors in students from the implementation area of "nutrition improvement programme for rural compulsory eduaction students"[D]. Beijing: Chinese Center for Disesse Contril and Prevention, 2016. [18] NEAD K G, HALTERMAN J S, KACZOROWSKI J M, et al. Overweight children and adolescents: a risk group for iron deficiency[J]. Pediatrics, 2004, 114(1): 104-108. doi: 10.1542/peds.114.1.104 [19] MAHUMD M A, SPIGT M, MULUGETA BEZABIH A, et al. Risk factors for intestinal parasitosis, anaemia, and malnutrition among school children in Ehiopia[J]. Pathog Glob Health, 2013, 107(2): 58-65. doi: 10.1179/2047773213Y.0000000074 [20] 李杨. 吉林省小学生营养状况及其影响因素分析[D]. 长春: 长春中医药大学, 2021.LI Y. Study on the nutritional status and related influencing factors of pupils in Jilin Province[D]. Changchun: Changchun Unmersity of Chinese Medicine, 2021. [21] HEATHER D, BATES H M, MCCARGAR L J. Assessment of iron status in adolescents: dietary, biochemical and lifestyle determinants[J]. J Adolesc Health Offic Publicat Soc Adolesc Med, 2005, 37(1): 75. -


 点击查看大图
点击查看大图
计量
- 文章访问数: 385
- HTML全文浏览量: 226
- PDF下载量: 35
- 被引次数: 0