


Trends in the asthma burden among children and adolescents in China from 1990-2019
-
摘要:
目的 探索1990—2019年中国儿童青少年哮喘疾病负担变化趋势,为开展防控工作提供参考。 方法 基于2019年全球疾病负担研究,利用Joinpoint回归分析性别和年龄别哮喘疾病负担动态变化,与各级社会人口指数(SDI)国家平均水平比较; 并分析归因哮喘疾病负担的变化。 结果 标化1~19岁哮喘伤残调整寿命年(DALYs)率1990—2005年间先小幅降低后快速降低,由158.55/10万降至88.59/10万。其中,1990—1996年年度变化百分比(APC)为-1.7%,1996—2005年APC为-5.7%。2005—2017年DALYs率先缓慢升高后快速升高,2017—2019年DALYs率由176.18/10万降为126.79/10万。男生哮喘疾病负担高于女生,5~9岁组哮喘DALYs率高于其他年龄组。中国儿童青少年哮喘标化DALYs率在不同SDI国家中处于较低水平。此外,归因于高体质量指数的哮喘DALYs率呈升高趋势,1~4岁组年度平均变化百分比(AAPC)为2.9%,其他年龄组AAPC均为4.2%;15~19岁组归因于职业性致喘物的DALYs率呈降低趋势,AAPC为-2.5%。 结论 中国儿童青少年哮喘疾病负担较低,有性别和年龄别差异,变化呈“降低—升高—降低”趋势。应重点关注男生和5~9岁儿童哮喘防治,加强对肥胖和职业性致喘物等危险因素的干预。 Abstract:Objective To explore trends in the asthma burden among Chinese children and adolescents 1-19 years old during 1990-2019. Methods Based on data from the 2019 Global Burden of Disease Study, joinpoint regression was used to analyze the dynamic changes in the gender-and age-specific asthma burden, and the asthma burden in China was compared with countries that have different socio-demographic indices(SDI). In addition, trends in asthma burden attributed to different risk factors were also investigated. Results The asthma burden decreased slightly from 1990 to 1996 [annual percent change (APC)=-1.7%], then rapidly decreased from 1996 to 2005 (APC=-5.7%). The age-standardized disability adjusted life years (DALYs) rate decreased from 158.55/100 000 to 88.59/100 000 in patients 1-19 years of age. From 2005 to 2017, the DALYs rate for asthma increased slowly, then rapidly. In 2017, the DALYs rate peaked at 176.18/100 000, then decreased to 126.79/100 000 in 2019. The burden of asthma in boys was higher than girls, and the DALYs rate for asthma in the group 5-9 years of age was higher than the remaining age groups. Furthermore, the age-standardized DALYs rate for asthma among Chinese children and adolescents was relatively low among countries with a different SDI. In addition, the DALYs rate attributed to high body mass index increased in all age groups in China. Specifically, the average APC (AAPC) was 2.9% in group 1-4 years of age and the AAPC was 4.2% in the remaining age groups. The DALYs rate attributed to occupational asthmagens in the group 15-19 years of age decreased from 1990 to 2019 and the AAPC was -2.5%. Conclusion The asthma burden was relatively low among Chinese children and adolescents, and there were gender and age differences. The gender-and age-specific DALYs rate for asthma had a tendency to decrease, increase, then decrease. More attention should be paid to boys and the group 5-9 years of age, and strengthen the intervention of obesity and occupational asthmagens. -
Key words:
- Asthma /
- Regression analysis /
- Child /
- Adolescent
1) 利益冲突声明 所有作者声明无利益冲突。 -

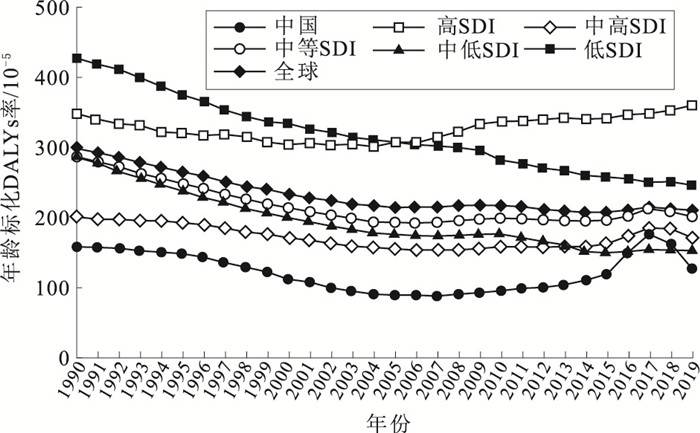
图 1 1990—2019年不同SDI水平地区儿童青少年年龄标化哮喘DALYs率变化趋势
Figure 1. Trends in age-standardized DALYs rate of asthma in the children and adolescents from 1990 to 2019 categorized by socio-demographic index

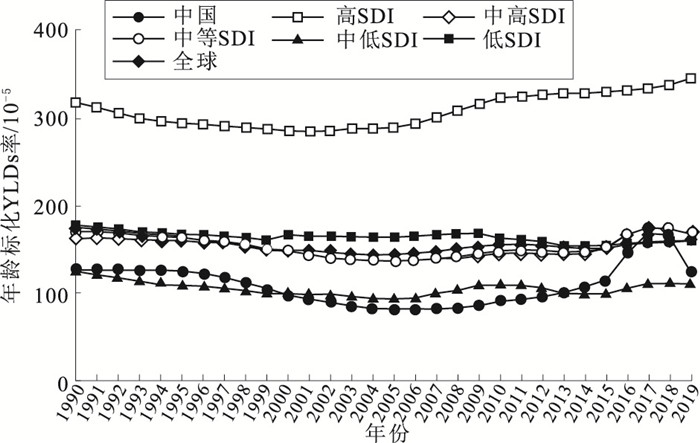
图 2 1990—2019年不同SDI水平地区儿童青少年年龄标化哮喘YLDs率变化趋势
Figure 2. Trends in age-standardized YLDs rate of asthma in the children and adolescents from 1990 to 2019 categorized by socio-demographic index

图 3 1990—2019年不同SDI水平地区儿童青少年年龄标化哮喘YLLs率变化趋势
Figure 3. Trends in age-standardized YLLs rate of asthma in the children and adolescents from 1990 to 2019 categorized by socio-demographic index
表 1 2019年中国不同年龄和性别儿童青少年哮喘疾病负担/10-5
Table 1. Burden of asthma among Chinese children and adolescents in 2019 categorized by age and sex/100 000
性别 年龄/岁 DALYs率 YLDs率 YLLs率 男 1~4 143.94(72.06~265.92) 140.87(69.16~262.78) 3.07(1.88~4.94) 5~9 204.74(104.50~376.61) 202.81(102.82~373.86) 1.93(1.35~2.76) 10~14 134.18(72.17~232.28) 132.05(70.24~230.03) 2.13(1.58~2.96) 15~19 85.39(45.43~147.47) 82.88(42.49~144.88) 2.51(1.81~3.63) 1~19 142.82(142.22~143.42)a 140.44(139.85~141.04)a 2.38(2.30~2.46)a 女 1~4 109.74(55.11~200.48) 107.26(52.02~198.21) 2.49(1.71~3.63) 5~9 146.85(73.29~271.67) 145.65(72.32~270.56) 1.20(0.92~1.70) 10~14 100.69(52.31~176.66) 99.31(51.30~175.27) 1.38(1.05~1.92) 15~19 72.90(38.80~125.99) 70.47(35.66~123.87) 2.43(1.72~3.39) 1~19 107.97(107.40~108.53)a 106.13(105.57~106.60)a 1.84(1.77~1.91)a 合计 1~4 128.15(64.07~235.68) 125.35(61.92~232.81) 2.80(1.90~4.06) 5~9 178.14(90.50~329.02) 176.55(89.03~327.38) 1.59(1.20~2.21) 10~14 118.86(63.16~205.74) 117.07(61.28~204.28) 1.79(1.41~2.43) 15~19 79.56(42.34~137.71) 77.09(39.38~135.54) 2.47(1.95~3.35) 1~19 126.79(126.37~127.20) 124.66(124.24~125.07) 2.13(2.08, 2.18) 注:()内数字为95%UI,a表示在男生和女生间异质性P < 0.01。  下载: 导出CSV
下载: 导出CSV
-
[1] 刘传合, 洪建国, 尚云晓, 等. 中国16城市儿童哮喘患病率20年对比研究[J]. 中国实用儿科杂志, 2015, 30: 596-600. https://www.cnki.com.cn/Article/CJFDTOTAL-ZSEK201508011.htmLIU C H, HONG J G, SHANG Y X, et al. Comparison of asthma prevalence in children from 16 cities of China in 20 years[J]. Chin J Practic Pediatr, 2015, 30: 596-600. https://www.cnki.com.cn/Article/CJFDTOTAL-ZSEK201508011.htm [2] PIJNENBURG M W, FLEMING L. Advances in understanding and reducing the burden of severe asthma in children[J]. Lancet Respir Med, 2020, 8(10): 1032-1044. doi: 10.1016/S2213-2600(20)30399-4 [3] FUCHS O, BAHMER T, RABE K F, et al. Asthma transition from childhood into adulthood[J]. Lancet Respir Med, 2017, 5(3): 224-234. doi: 10.1016/S2213-2600(16)30187-4 [4] HAYDEN L P, CHO M H, RABY B A, et al. Childhood asthma is associated with COPD and known asthma variants in COPD Gene: a genome-wide association study[J]. Respir Res, 2018, 19(1): 209. doi: 10.1186/s12931-018-0890-0 [5] LI X, SONG P, ZHU Y, et al. The disease burden of childhood asthma in China: a systematic review and Meta-analysis[J]. J Glob Health, 2020, 10(1): 010801. doi: 10.7189/jogh.10.010801 [6] KIM H J, FAY M P, FEUER E J, et al. Permutation tests for joinpoint regression with applications to cancer rates[J]. Stat Med, 2000, 19(3): 335-351. doi: 10.1002/(SICI)1097-0258(20000215)19:3<335::AID-SIM336>3.0.CO;2-Z [7] GBD 2019 Diseases and Injuries Collaborators. Global burden of 369 diseases and injuries in 204 countries and territories, 1990-2019: a systematic analysis for the Global Burden of Disease Study 2019[J]. Lancet, 2020, 396(10258): 1204-1222. doi: 10.1016/S0140-6736(20)30925-9 [8] GBD 2019 Risk Factors Collaborators. Global burden of 87 risk factors in 204 countries and territories, 1990-2019: a systematic analysis for the Global Burden of Disease Study 2019[J]. Lancet, 2020, 396(10258): 1223-1249. doi: 10.1016/S0140-6736(20)30752-2 [9] 李辉章, 杜灵彬. Joinpoint回归模型在肿瘤流行病学时间趋势分析中的应用[J]. 中华预防医学杂志, 2020, 54(8): 908-912.LI H Z, DU L B. Application of Joinpoint regression model in cancer epidemiological time trend analysis[J]. Chin J Prev Med, 2020, 54(8): 908-912. [10] COLE T J, LOBSTEIN T. Extended international (IOTF) body mass index cut-offs for thinness, overweight and obesity[J]. Pediatr Obes, 2012, 7(4): 284-294. doi: 10.1111/j.2047-6310.2012.00064.x [11] 李丽香, 林淑珍, 张任攀, 等. 中国农村儿童哮喘患病情况的Meta分析[J]. 中国当代儿科杂志, 2020, 22(4): 380-386. https://www.cnki.com.cn/Article/CJFDTOTAL-DDKZ202004020.htmLI L X, LIN S Z, ZHANG R P, et al. Prevalence of pediatric asthma in the rural areas of China: a meta analysis[J]. Chin J Contemp Pediatr, 2020, 22(4): 380-386. https://www.cnki.com.cn/Article/CJFDTOTAL-DDKZ202004020.htm [12] 刘传合, 洪建国, 尚云晓, 等. 第三次中国城市儿童哮喘流行病学调查[J]. 中华儿科杂志, 2013, 51(10): 729-735.LIU C H, HONG J G, SHANG Y X, et al. Third nationwide survey of childhood asthma in urban areas of China[J]. Chin J Pediatr, 2013, 51(10): 729-735. [13] ZAHRAN H, BAILEY C, DAMON S, et al. Vital signs: asthma in children-United States, 2001-2016[J]. MMWR, 2018, 67(5): 149-155. [14] SHAH R, NEWCOMB D C. Sex bias in asthma prevalence and pathogenesis[J]. Front Immunol, 2018, 9: 2997. doi: 10.3389/fimmu.2018.02997 [15] 袁金娜, 金冰涵, 斯淑婷, 等. 2009至2019年6~15岁中国儿童超重和肥胖趋势分析[J]. 中华儿科杂志, 2021, 59(11): 935-941.YUAN J N, JIN B H, SI S T, et al. Changing prevalence of overweight and obesity among Chinese children aged 6-15 from 2009-2019[J]. Chin J Pediatr, 2021, 59(11): 935-941. [16] 刘婷婷, 齐金蕾, 殷菊, 等. 2008—2018年中国0~19岁人群哮喘死亡现状及变化趋势分析[J]. 中华实用儿科临床杂志, 2021, 36(6): 471-475.LIU T T, QI J L, YIN J, et al. Analysis of death status and change trend of asthma among Chinese people aged 0-19 years from 2008 to 2018[J]. Chin J Practic Pediatr, 2021, 36(6): 471-475. [17] GUAN W J, ZHENG X Y, CHUNG K F, et al. Impact of air pollution on the burden of chronic respiratory diseases in China: time for urgent action[J]. Lancet, 2016, 388(10054): 1939-1951. doi: 10.1016/S0140-6736(16)31597-5 [18] ASHER M I, GARCÍA-MARCOS L, PEARCE N E, et al. Trends in worldwide asthma prevalence[J]. Eur Respir J, 2020, 56(6): 2002094. doi: 10.1183/13993003.02094-2020 [19] GBD 2015 Healthcare Access And Quality Collaborators. Healthcare Access and Quality Index based on mortality from causes amenable to personal health care in 195 countries and territories, 1990-2015: a novel analysis from the Global Burden of Disease Study 2015[J]. Lancet, 2017, 390(10091): 231-266. [20] PAPI A, BRIGHTLING C, PEDERSEN S E, et al. Asthma[J]. Lancet, 2018, 391(10122): 783-800. [21] GBD 2015 Chronic Respiratory Disease Collaborators. Global, regional, and national deaths, prevalence, disability-adjusted life years, and years lived with disability for chronic obstructive pulmonary disease and asthma, 1990-2015: a systematic analysis for the Global Burden of Disease Study 2015[J]. Lancet Respir Med, 2017, 5(9): 691-706. [22] MALDEN S, GILLESPIE J, HUGHES A, et al. Obesity in young children and its relationship with diagnosis of asthma, vitamin D deficiency, iron deficiency, specific allergies and flat-footedness: a systematic review and Meta-analysis[J]. Obes Rev, 2021, 22(3): e13129. [23] AHMADIZAR F, VIJVERBERG S J, ARETS H G, et al. Childhood obesity in relation to poor asthma control and exacerbation: a Meta-analysis[J]. Eur Respir J, 2016, 48(4): 1063-1073. [24] 张娜, 马冠生. 《中国儿童肥胖报告》解读[J]. 营养学报, 2017, 39(6): 530-534. https://www.cnki.com.cn/Article/CJFDTOTAL-YYXX201706005.htmZHANG N, MA G S. Interpretation of report on childhood obesity in China[J]. J Nutr, 2017, 39(6): 530-534. https://www.cnki.com.cn/Article/CJFDTOTAL-YYXX201706005.htm [25] 房红芸, 翟屹, 赵丽云, 等. 中国6~17岁儿童青少年超重肥胖流行特征[J]. 中华流行病学杂志, 2018, 39(6): 724-727.FANG H Y, ZHAI Y, ZHAO L Y, et al. Epidemiological characteristics of overweight and obesity in Chinese children and adolescents aged 6-17 years[J]. Chin J Epidemiol, 2018, 39(6): 724-727. [26] 陈贻珊, 张一民, 孔振兴, 等. 我国儿童青少年超重、肥胖流行现状调查[J]. 中华疾病控制杂志, 2017, 21(9): 866-869, 878. https://www.cnki.com.cn/Article/CJFDTOTAL-JBKZ201709002.htmCHENG Y S, ZHANG Y M, KONG Z X, et al. The prevalence of overweight and obesity in children and adolescents in China[J]. Chin J Dis Control Prev, 2017, 21(9): 866-869, 878. https://www.cnki.com.cn/Article/CJFDTOTAL-JBKZ201709002.htm [27] 高珊珊, 李侠, 宋占帅. 职业性低分子质量致喘物研究进展[J]. 中国职业医学, 2016, 43(3): 384-386, 392. https://www.cnki.com.cn/Article/CJFDTOTAL-XYYX201603032.htmGAO S S, LI X, SONG Z S. Research progress on occupational low molecular weight asthma inducing agens[J]. Chin Occup Med, 2016, 43(3): 384-386, 392. https://www.cnki.com.cn/Article/CJFDTOTAL-XYYX201603032.htm [28] LI L, HART J E, COULL B A, et al. Effect of residential greenness and nearby parks on respiratory and allergic diseases among middle school adolescents in a Chinese city[J]. Int J Environ Res Public Health, 2019, 16(6): 991. [29] ZENG X W, LOWE A J, LODGE C J, et al. Greenness surrounding schools is associated with lower risk of asthma in schoolchildren[J]. Environ Int, 2020, 143: 105967. [30] YU H, ZHOU Y, WANG R, et al. Associations between trees and grass presence with childhood asthma prevalence using deep learning image segmentation and a novel green view index[J]. Environ Pollut, 2021, 286: 117582. [31] LAMBERT K A, BOWATTE G, THAM R, et al. Residential greenness and allergic respiratory diseases in children and adolescents: a systematic review and Meta-analysis[J]. Environ Res, 2017, 159: 212-221. [32] ISLAM M Z, JOHNSTON J, SLY P D. Green space and early childhood development: a systematic review[J]. Rev Environ Health, 2020, 35(2): 189-200. [33] HARTLEY K, RYAN P, BROKAMP C, et al. Effect of greenness on asthma in children: a systematic review[J]. Public Health Nurs, 2020, 37(3): 453-460. [34] PARMES E, PESCE G, SABEL C E, et al. Influence of residential land cover on childhood allergic and respiratory symptoms and diseases: evidence from 9 European cohorts[J]. Environ Res, 2020, 183: 108953. -


 点击查看大图
点击查看大图
计量
- 文章访问数: 1096
- HTML全文浏览量: 426
- PDF下载量: 72
- 被引次数: 0