


Study on the growth curve of uncorrected visual acuity of children and adolescents with relative safe refractive range
-
摘要:
目的 分析3~18岁屈光相对安全范围儿童青少年裸眼视力分布,为研制不同年龄段儿童青少年裸眼视力的生长曲线和参考值范围、制定视力异常转诊界值提供参考。 方法 通过整群抽样的方法,选取上海市9 146名3~18岁儿童青少年进行裸眼视力、散瞳验光、裂隙灯等眼科检查,采用LMS法拟合屈光相对安全范围儿童青少年裸眼视力的百分位数和生长曲线,同时分析各年龄组裸眼视力筛查屈光异常的ROC曲线下面积及不同界值的灵敏度和特异度。 结果 儿童青少年裸眼视力呈偏态分布,中位数为4.8。其中屈光相对安全范围儿童青少年4 675名,裸眼视力中位数为4.9。LMS拟合曲线显示,裸眼视力在低年龄段随年龄增长而提高,6~10岁时逐渐稳定至最佳水平。P50在3~4岁为4.8,5~8岁为4.9,≥9岁均为5.0。裸眼视力预测屈光异常的ROC曲线下面积随年龄的增加而提高,3岁时仅为0.55(95%CI=0.50~0.61),12~18岁时最高[0.95(95%CI=0.94~0.96)]。3~6岁以P25为转诊界值时约登指数最高,7岁及以上以P10为界值时约登指数最高。随着界值的增加,灵敏度提高,特异度降低。 结论 裸眼视力随年龄增长先提升,6~10岁后逐渐稳定至视力最佳水平。年龄越大,裸眼视力指标筛查屈光异常的效果越好。建议根据年龄设置儿童青少年裸眼视力异常转诊界值,各年龄段可根据筛查目的选择P25~P75为转诊界值。 Abstract:Objective To analyze the distribution of uncorrected visual acuity in children and adolescents aged 3-18 years with relative safe refractive range, and to develop the growth curve and reference range of uncorrected visual acuity in children and adolescents of different ages, so as to provide reference for formulating the referral threshold for myopia screening practice. Methods Using cluster sampling method, 9 146 children and adolescents aged 3-18 years old in Shanghai were selected for uncorrected visual acuity, cycloplegic refraction, slit lamp and other ophthalmic examinations, and the percentiles and growth curve of uncorrected visual acuity of children and adolescents in the relative safe refractive range were fitted by LMS method. Besides, the area under the ROC curve and the sensitivity and specificity of different cut-off values were analyzed. Results The uncorrected visual acuity was skewed, with a median of 4.8. There were 4 675 individuals with safe refraction, the median of uncorrected visual acuity in which was 4.9. The LMS curve showed that the uncorrected visual acuity increased with age in the lower age group, and gradually stabilized to the best level at the age of 6-10. P50 was 4.8 in 3-4 years old, 4.9 in 5-8 years old, 5.0 in 9 years old and above. The area under ROC curve of uncorrected visual acuity predicting refractive abnormality increased with age, with the lowest value of 0.55(95%CI=0.50-0.61) at 3 years old and the highest value of 0.95 (95%CI=0.94-0.96) at 12-18 years old. The Youden index was the highest for P25 at 3-6 years old, and the highest for P10 at 7 years old and above. With the increase of the cut-off value, the sensitivity increased and the specificity decreased. Conclusion The uncorrected visual acuity increases gradually with age, and reaches the best level after 6-10 years old. The screening effect of uncorrected visual acuity predicting refractive abnormality increased with age. It is suggested that the referral threshold of children and adolescents with abnormal uncorrected visual acuity should be set according to their ages, and P25-P75 can be selected according to the screening purposes. -
Key words:
- Refraction, ocular /
- Growth and development /
- ROC curve /
- Child /
- Adolescent
-

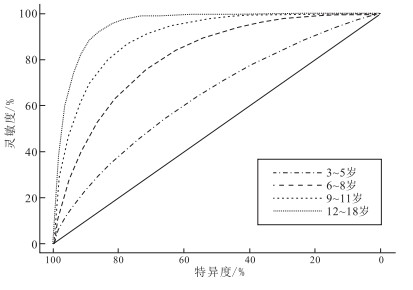
图 1 各年龄组儿童青少年裸眼视力筛查异常的ROC曲线
Figure 1. ROC curve analysis of uncorrected visual acuity screening for abnormal refraction in different age groups
表 1 屈光相对安全范围儿童青少年裸眼视力分布
Table 1. Distribution of uncorrected visual acuity in children and adolescents with relative safe refraction
年龄/岁 人数 P3 P10 P25 P50 P75 P90 P97 均值 3 225 4.6 4.6 4.7 4.8 4.8 4.9 5.0 4.8 4 377 4.6 4.7 4.8 4.8 4.9 4.9 5.0 4.8 5 411 4.6 4.8 4.8 4.9 4.9 4.9 5.0 4.9 6 803 4.7 4.8 4.8 4.9 4.9 5.0 5.0 4.9 7 828 4.7 4.8 4.9 4.9 5.0 5.0 5.0 4.9 8 711 4.8 4.8 4.9 4.9 5.0 5.0 5.1 5.0 9 544 4.8 4.9 4.9 5.0 5.0 5.0 5.1 5.0 10 309 4.8 4.8 4.9 5.0 5.0 5.0 5.1 5.0 11 184 4.8 4.9 4.9 5.0 5.0 5.0 5.1 5.0 12 104 4.8 4.9 4.9 5.0 5.0 5.0 5.1 5.0 13 75 4.8 4.9 5.0 5.0 5.0 5.1 5.1 5.0 14 43 4.8 4.9 4.9 5.0 5.0 5.1 5.1 5.0 15 26 4.8 4.8 4.9 5.0 5.0 5.0 5.1 5.0 16~18 35 4.8 4.8 5.0 5.0 5.0 5.1 5.1 5.0  下载: 导出CSV
下载: 导出CSV
表 2 基于LMS法拟合的屈光相对安全范围儿童青少年各年龄段裸眼视力百分位数值
Table 2. Percentiles of uncorrected visual acuity among children and adolescents with relative safe refraction in different age groups based on LMS method
年龄/岁 人数 P3 P10 P25 P50 P75 P90 P97 3 225 4.6 4.7 4.7 4.8 4.8 4.9 4.9 4 377 4.6 4.7 4.8 4.8 4.9 4.9 5.0 5 411 4.7 4.8 4.8 4.9 4.9 5.0 5.0 6 803 4.7 4.8 4.8 4.9 4.9 5.0 5.0 7 828 4.7 4.8 4.9 4.9 5.0 5.0 5.1 8 711 4.7 4.8 4.9 4.9 5.0 5.0 5.1 9 544 4.8 4.8 4.9 5.0 5.0 5.1 5.1 10 309 4.8 4.9 4.9 5.0 5.0 5.1 5.1 11 184 4.8 4.9 4.9 5.0 5.0 5.1 5.1 12 104 4.8 4.9 4.9 5.0 5.0 5.1 5.1 13 75 4.8 4.9 4.9 5.0 5.0 5.1 5.1 14 43 4.8 4.9 4.9 5.0 5.0 5.1 5.1 15 26 4.8 4.9 4.9 5.0 5.0 5.1 5.1 16~18 35 4.8 4.9 4.9 5.0 5.0 5.1 5.1
下载: 导出CSV
表 3 不同年龄组屈光相对安全范围儿童青少年分性别裸眼视力分布的敏感性分析
Table 3. Analysis of the distribution of uncorrected visual acuity in children and adolescents with relative safe refractive range in different genders
年龄/岁 男生 女生 P3 P10 P25 P50 P75 P90 P97 P3 P10 P25 P50 P75 P90 P97 3 4.6 4.7 4.7 4.8 4.8 4.9 4.9 4.6 4.7 4.7 4.8 4.8 4.9 4.9 4 4.6 4.7 4.8 4.8 4.9 4.9 5.0 4.6 4.7 4.8 4.8 4.9 4.9 5.0 5 4.6 4.8 4.8 4.9 4.9 5.0 5.0 4.7 4.7 4.8 4.9 4.9 5.0 5.0 6 4.7 4.8 4.9 4.9 4.9 5.0 5.0 4.7 4.8 4.8 4.9 4.9 5.0 5.0 7 4.7 4.8 4.9 4.9 5.0 5.0 5.1 4.7 4.8 4.9 4.9 5.0 5.0 5.1 8 4.7 4.8 4.9 5.0 5.0 5.0 5.1 4.7 4.8 4.9 4.9 5.0 5.0 5.1 9 4.7 4.8 4.9 5.0 5.0 5.1 5.1 4.8 4.8 4.9 5.0 5.0 5.0 5.1 10 4.7 4.9 4.9 5.0 5.0 5.1 5.1 4.8 4.9 4.9 5.0 5.0 5.1 5.1 11 4.7 4.9 4.9 5.0 5.0 5.1 5.1 4.8 4.9 4.9 5.0 5.0 5.1 5.1 12 4.8 4.9 4.9 5.0 5.0 5.1 5.1 4.8 4.9 4.9 5.0 5.0 5.1 5.1 13 4.8 4.9 4.9 5.0 5.0 5.1 5.1 4.8 4.9 4.9 5.0 5.0 5.1 5.1 14 4.8 4.9 4.9 5.0 5.0 5.1 5.1 4.8 4.9 4.9 5.0 5.0 5.1 5.1 15 4.8 4.9 4.9 5.0 5.0 5.1 5.1 4.8 4.9 4.9 5.0 5.0 5.1 5.1 16~18 4.8 4.9 4.9 5.0 5.0 5.1 5.1 4.8 4.9 4.9 5.0 5.0 5.1 5.1
下载: 导出CSV
表 4 各年龄组不同屈光定义下儿童青少年裸眼视力分布的敏感性分析
Table 4. Analysis of uncorrected visual acuity distribution of children and adolescents under different refractive definitions
年龄/岁 SE[0, 1]D SE[0.5, 2]D SE[-0.5, 0.5]D P3 P10 P25 P50 P75 P90 P97 P3 P10 P25 P50 P75 P90 P97 P3 P10 P25 P50 P75 P90 P97 3 4.6 4.7 4.7 4.8 4.8 4.9 4.9 4.6 4.7 4.7 4.8 4.8 4.9 4.9 4.5 4.6 4.7 4.8 4.8 4.9 4.9 4 4.6 4.7 4.8 4.8 4.9 4.9 4.9 4.6 4.7 4.8 4.8 4.9 4.9 5.0 4.5 4.7 4.7 4.8 4.9 4.9 4.9 5 4.7 4.8 4.8 4.9 4.9 4.9 5.0 4.7 4.8 4.8 4.9 4.9 5.0 5.0 4.6 4.7 4.8 4.8 4.9 4.9 5.0 6 4.7 4.8 4.9 4.9 4.9 5.0 5.0 4.7 4.8 4.8 4.9 4.9 5.0 5.0 4.6 4.7 4.8 4.9 4.9 5.0 5.0 7 4.7 4.8 4.9 4.9 5.0 5.0 5.1 4.7 4.8 4.9 4.9 5.0 5.0 5.1 4.6 4.8 4.8 4.9 5.0 5.0 5.0 8 4.7 4.8 4.9 5.0 5.0 5.0 5.1 4.7 4.8 4.9 5.0 5.0 5.0 5.1 4.6 4.8 4.9 4.9 5.0 5.0 5.1 9 4.8 4.9 4.9 5.0 5.0 5.0 5.1 4.8 4.8 4.9 5.0 5.0 5.1 5.1 4.7 4.8 4.9 4.9 5.0 5.0 5.1 10 4.8 4.9 4.9 5.0 5.0 5.1 5.1 4.8 4.9 4.9 5.0 5.0 5.1 5.1 4.7 4.8 4.9 4.9 5.0 5.0 5.1 11 4.8 4.9 4.9 5.0 5.0 5.1 5.1 4.8 4.9 4.9 5.0 5.0 5.1 5.1 4.7 4.8 4.9 4.9 5.0 5.0 5.1 12 4.8 4.9 4.9 5.0 5.0 5.1 5.1 4.8 4.9 4.9 5.0 5.0 5.1 5.1 4.7 4.8 4.9 4.9 5.0 5.0 5.1 13 4.8 4.9 4.9 5.0 5.0 5.1 5.1 4.8 4.9 4.9 5.0 5.0 5.1 5.1 4.7 4.8 4.9 4.9 5.0 5.0 5.1 14 4.8 4.9 4.9 5.0 5.0 5.1 5.1 4.8 4.9 4.9 5.0 5.0 5.1 5.1 4.7 4.8 4.9 4.9 5.0 5.0 5.1 15 4.8 4.9 4.9 5.0 5.0 5.1 5.1 4.8 4.9 4.9 5.0 5.0 5.1 5.1 4.7 4.8 4.9 4.9 5.0 5.0 5.1 16~18 4.8 4.9 4.9 5.0 5.0 5.1 5.1 4.8 4.9 4.9 5.0 5.0 5.1 5.1 4.7 4.8 4.9 4.9 5.0 5.0 5.1
下载: 导出CSV
表 5 各年龄组儿童青少年裸眼视力筛查屈光异常的ROC曲线下面积及不同界值的灵敏度和特异度分析
Table 5. Area under ROC curve as well as the sensitivity and specificity analysis of different cut-off values of uncorrected visual acuity for screening abnormal refraction in different age groups
年龄/岁 曲线下面积(95%CI) ≤P10 ≤P25 ≤P50 ≤P75 ≤P90 界值 灵敏度/% 特异度/% 约登指数/% 界值 灵敏度/% 特异度/% 约登指数/% 界值 灵敏度/% 特异度/% 约登指数/% 界值 灵敏度/% 特异度/% 约登指数/% 界值 灵敏度/% 特异度/% 约登指数/% 3 0.55(0.50~0.61) 4.7 44.68 64.89 9.57 4.7 44.68 64.89 9.57 4.8 91.49 12.89 4.38 4.8 91.49 12.89 4.38 4.9 96.81 6.67 3.48 4 0.67(0.63~0.71) 4.7 40.71 80.37 21.08 4.8 87.14 37.67 24.81 4.8 87.14 37.67 24.81 4.9 97.86 5.57 3.43 4.9 97.86 5.57 3.43 5 0.69(0.65~0.73) 4.8 72.55 57.66 30.21 4.8 72.55 57.66 30.21 4.9 98.04 7.06 5.10 4.9 98.04 7.06 5.10 5.0 100.00 0.00 0.00 6 0.72(0.70~0.75) 4.8 64.60 72.35 36.95 4.8 64.60 72.35 36.95 4.9 92.34 20.55 12.89 4.9 92.34 20.55 12.89 5.0 100.00 1.25 1.25 7 0.81(0.78~0.83) 4.8 67.33 81.28 48.61 4.9 91.67 38.53 30.20 4.9 91.67 38.53 30.20 5.0 100.00 1.57 1.57 5.0 100.00 1.57 1.57 8 0.86(0.83~0.88) 4.8 73.80 87.34 61.14 4.9 90.39 48.10 38.49 4.9 90.39 48.10 38.49 5.0 99.34 4.50 3.84 5.0 99.34 4.50 3.84 9 0.89(0.87~0.91) 4.8 72.73 94.30 67.03 4.9 89.39 64.34 53.73 5.0 98.86 6.25 5.11 5.0 98.86 6.25 5.11 5.1 100.00 0.55 0.55 10 0.91(0.89~0.93) 4.9 91.90 62.14 54.04 4.9 91.90 62.14 54.04 5.0 99.45 5.50 4.95 5.0 99.45 5.50 4.95 5.1 100.00 0.32 0.32 11 0.94(0.91~0.95) 4.9 92.46 71.20 63.66 4.9 92.46 71.20 63.66 5.0 99.50 8.15 7.65 5.0 99.50 8.15 7.65 5.1 100.00 1.09 1.09 12~18 0.95(0.94~0.96) 4.9 94.50 72.79 67.29 4.9 94.50 72.79 67.29 5.0 99.37 10.25 9.62 5.0 99.37 10.25 9.62 5.1 99.94 1.06 1.00
下载: 导出CSV
-
[1] MODJTAHEDI B S, ABBOTT R L, FONG D S, et al. Reducing the global burden of myopia by delaying the onset of myopia and reducing myopic progression in children[J]. Ophthalmology, 2021, 128(6): 816-826. doi: 10.1016/j.ophtha.2020.10.040 [2] NAIDOO K S, FRICKE T R, FRICK K D, et al. Potential lost productivity resulting from the global burden of myopia[J]. Ophthalmology, 2019, 126(3): 338-346. doi: 10.1016/j.ophtha.2018.10.029 [3] 国家卫生健康委员会. 2019年4月29日例行新闻发布会文字实录[A/OL]. [2019-04-29]. http://www.nhc.gov.cn/xcs/s7847/201904/e9117ea8b6b84f48962e84401d305292.shtml.National Health Commission of the People's Republic of China. Transcript of routine press conference on April 29, 2019[A/OL]. [2019-04-29]. http://www.nhc.gov.cn/xcs/s7847/201904/e9117ea8b6b84f48962e84401d305292.shtml. [4] 教育部. 综合防控儿童青少年近视实施方案[A]. 2018-08-30.Ministry of Education of the People's Republic of China. Implementation plan for comprehensive prevention and control of myopia in children and adolescents[A]. 2018-8-30. [5] 褚仁远, 瞿小妹. 建立儿童屈光发育档案是预防近视的基础步骤[J]. 中华眼科杂志, 2009, 45(7): 577-579. doi: 10.3760/cma.j.issn.0412-4081.2009.07.001CHU R Y, QU X M. The basic step to prevent myopia is to set up children's refractive development files[J]. Chin J Ophthalmol, 2009, 45(7): 577-579. doi: 10.3760/cma.j.issn.0412-4081.2009.07.001 [6] 教育部. 全国学生体质健康监测网络工作实施方案[A/OL]. [2002-03-21]. http://www.moe.gov.cn/jyb_xxgk/gk_gbgg/moe_0/moe_8/moe_25/tnull_285.html.Ministry of Education of the People's Republic of China. Implementation plan of national student physical health monitoring network[A/OL]. [2002-03-21]. http://www.moe.gov.cn/jyb_xxgk/gk_gbgg/moe_0/moe_8/moe_25/tnull_285.html. [7] 国家卫生健康委疾病预防控制局. 国家卫生健康委办公厅教育部办公厅财政部办公厅关于开展2018年儿童青少年近视调查工作的通知[A/OL]. [2018-10-26]. http://www.nhc.gov.cn/jkj/s5898bm/201810/08e2b45092d346a8a8c960d3e3d98b62.shtml.Bureau of Disease Control and Prevention of the National Health Commission. Notice of the General Office of the National Health Commission, the General Office of the Ministry of Education and the General Office of the Ministry of Finance on the investigation of myopia among children and adolescents in 2018[A/OL]. [2018-10-26]. http://www.nhc.gov.cn/jkj/s5898bm/201810/08e2b45092d346a8a8c960d3e3d98b62.shtml. [8] 国家卫生健康委员会. 中小学生屈光不正筛查规范WS/T 663—2020[S]. 2020-06-01.National Health Commission of the People's Republic of China. Screening criterion of ametropia in primary and middle school students WS/T 663—2020[S]. 2020-06-01. [9] 国家食品药品监督管理局. 眼科仪器: 验光仪ISO 10342[S]. 北京, 2009.State Food and Drug Administration of the people's Republic of China. Ophthalmic instruments: refractors ISO 10342[S]. Beijing, 2009. [10] LUN M X, GUI C, ZHANG L, et al. Application of the LMS method of constructing fetal reference charts: comparison with the original method[J]. J Matern Fetal Neonatal Med, 2021, 34(3): 395-402. doi: 10.1080/14767058.2019.1608942 [11] 邵子瑜, 孙瑜, 李培培, 等. 低出生体重儿婴儿期体格生长指标参考值偏度系数-中位数-变异系数法研究[J]. 中华疾病控制杂志, 2020, 24(10): 1195-1201. https://www.cnki.com.cn/Article/CJFDTOTAL-JBKZ202010018.htmSHAO Z Y, SUN Y, LI P P, et al. Lambda-mu-sigma method (LMS) study on the physical growth reference standard of low birth weight infant[J]. Chin J Dis Control Prevent, 2020, 24(10): 1195-1201. https://www.cnki.com.cn/Article/CJFDTOTAL-JBKZ202010018.htm [12] ZVONAR M, TEFAN L, KASOVI M. Percentile curves for body-mass index, waist circumference, waist-to-height ratio and waist-to-height ratio(exp) in croatian adolescents[J]. Int J Environ Res Public Health, 2019, 16(11): 1920. doi: 10.3390/ijerph16111920 [13] 郭敏. 儿童青少年肥胖的患病率及生长发育曲线绘制[D]. 天津: 天津医科大学, 2020.GUO M. Prevalence and growth curve of obesity in children and adolescents[D]. Tianjin: Tianjin Medical University, 2020. [14] 王利华. 重视儿童常见眼病诊疗中的过度医疗问题[J]. 中华眼科杂志, 2016, 52(8): 561-564. doi: 10.3760/cma.j.issn.0412-4081.2016.08.001WANG L H. Pay attention to the problem of over treatment in the diagnosis and treatment of common eye diseases in children[J]. Chin J Ophthalmol, 2016, 52(8): 561-564. doi: 10.3760/cma.j.issn.0412-4081.2016.08.001 [15] LEAT S J, YADAV N K, IRVING E L. Development of visual acuity and contrast sensitivity in children[J]. J Optom, 2009, 2(1): 19-26. doi: 10.3921/joptom.2009.19 [16] 国家卫生和计划生育委员会. 儿童眼及视力保健技术规范[J]. 中国乡村医药, 2013, 20(12): 85-87. doi: 10.3969/j.issn.1006-5180.2013.12.050National Health and Family Planning Commission the People's Republic of China. Technical specification for children's eye and vision care[J]. Chin J Rural Med Pharm, 2013, 20(12): 85-87. doi: 10.3969/j.issn.1006-5180.2013.12.050 [17] 中华医学会眼科学分会斜视与小儿眼科学组. 弱视诊断专家共识(2011年)[J]. 中华眼科杂志, 2011, 47(8): 768. doi: 10.3760/cma.j.issn.0412-4081.2011.08.027Strabismus and Pediatric Ophthalmology Group, Ophthalmology Branch, Chinese Medical Association. Expert consensus on amblyopia diagnosis(2011)[J]. Chin J Ophthalmol, 2011, 47(8): 768. doi: 10.3760/cma.j.issn.0412-4081.2011.08.027 [18] 金迦力, 何鲜桂, 陆丽娜, 等. 筛查在预防儿童近视中的作用评价[J]. 中国学校卫生, 2013, 34(8): 1015-1017. http://www.cjsh.org.cn/article/id/zgxxws201308049JIN J L, HE X G, LU L N, et al. Evaluation of the role of screening in the prevention of myopia in children[J]. Chin J Sch Health, 2013, 34(8): 1015-1017. http://www.cjsh.org.cn/article/id/zgxxws201308049 -

 点击查看大图
点击查看大图
计量
- 文章访问数: 700
- HTML全文浏览量: 438
- PDF下载量: 85
- 被引次数: 0